
Purpose of This Guideline
Date of current publication: October 16, 2025
Lead authors: Rona M. Vail, MD, AAHIVS; Aviva Cantor, DMSc, PA, AAHIVS
Writing group: Sanjiv S. Shah, MD, MPH, AAHIVS; Steven M. Fine, MD, PhD; Joseph P. McGowan, MD, FACP, FIDSA, AAHIVS; Samuel T. Merrick, MD, FIDSA; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Anne K. Monroe, MD, MSPH; Jessica Rodrigues, MPH, MS; Christopher J. Hoffmann, MD, MPH, MSc, FACP; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: October 10, 2019
HIV prevention with pre-exposure prophylaxis (PrEP) is the use of antiretroviral medications by individuals who do not have HIV to reduce their risk of acquiring HIV. PrEP is a cornerstone of HIV prevention and is strongly endorsed by New York State. However, it is underutilized, particularly by communities disproportionately affected by HIV.
The New York State Ending the Epidemic (ETE) initiative presents strategies to decrease HIV prevalence and end the AIDS epidemic in New York State. The third pillar of the 3-pillar ETE plan is facilitating access to PrEP as a proven strategy to prevent HIV acquisition among individuals at risk. Its inclusion as a pillar of this initiative emphasizes the safety and effectiveness of PrEP as an HIV prevention method. This guideline was developed by the Medical Care Criteria Committee of the NYSDOH AI Clinical Guidelines Program to help clinicians successfully start and continue PrEP for individuals at risk of acquiring HIV.
In support of the ETE initiative and to reduce new HIV infections in New York State, the goals of this guideline are to:
- Increase clinician awareness and knowledge of PrEP efficacy.
- Assist clinicians in identifying candidates for PrEP and increasing PrEP awareness, access, and uptake among individuals at risk of acquiring HIV through sexual and drug use exposures.
- Discuss barriers to PrEP access and encourage clinicians to assist PrEP candidates in reducing or eliminating these barriers.
- Provide clinicians with the information needed to help a PrEP candidate make the best choice regarding oral versus injectable PrEP and daily versus on-demand PrEP.
- Provide evidence-based recommendations for PrEP initiation, management, monitoring, and discontinuation.
Note on “experienced” HIV care providers: The NYSDOH AI Clinical Guidelines Program defines an “experienced HIV care provider” as a practitioner who has been accorded HIV Specialist status by the American Academy of HIV Medicine. Nurse practitioners (NPs) and licensed midwives who provide clinical care to individuals with HIV in collaboration with a physician may be considered experienced HIV care providers if all other practice agreements are met; NPs with more than 3,600 hours of qualifying experience do not require collaboration with a physician (8 NYCRR 79-5:1; 10 NYCRR 85.36; 8 NYCRR 139-6900). Physician assistants who provide clinical care to individuals with HIV under the supervision of an HIV Specialist physician may also be considered experienced HIV care providers (10 NYCRR 94.2).
Improving PrEP Equity, Uptake, and Persistence Through Structural Support and Patient-Centered Choice
PrEP uptake: Although new HIV infections and diagnoses have steadily declined in New York State, these decreases have not been uniform across all groups. Men who have sex with men (MSM), particularly young MSM, and people of color continue to be overrepresented among those newly infected and diagnosed with HIV NYSDOH 2023. Computer simulation modeling suggests that increased PrEP uptake will be the single largest contributor to further reductions in new HIV infections and key to ending the HIV epidemic in New York State Martin, et al. 2020. However, data indicate that people of color, cisgender women, and individuals accessing Medicaid, 3 groups overrepresented among people with HIV, are accessing PrEP at lower levels than other groups in whom the disease burden is high Ending the Epidemic Dashboard 2025. For example, in 2023, 20.9% of new HIV diagnoses in New York State were in cisgender women and people assigned female at birth NYSDOH 2023 but just 8% of all individuals who accessed PrEP in New York State were women Ending the Epidemic Dashboard 2025. When broken down by race, 43% of PrEP prescriptions were written for White individuals, 12% for Black individuals, 10% for Hispanic individuals, 27% for “unknown,” 4% for Asian/Pacific Islander individuals, and 4% for “other” individuals Ending the Epidemic Dashboard 2025.
Barriers to PrEP access, use, and persistence: PrEP uptake, adherence, and persistence vary widely across populations and are influenced by structural, care provider, and individual-level factors. Suboptimal awareness and acceptance of PrEP among at-risk individuals and their care providers remain key barriers to initiation Townes, et al. 2021; Bazzi, et al. 2018; Mayer, et al. 2018.
Among Black MSM, low perceived HIV risk, stigma, and medical mistrust rooted in systemic racism significantly impede PrEP use. Those unaware of PrEP often have lower HIV testing rates, limited HIV knowledge, and higher rates of transactional sex Russ, et al. 2021. Additional structural barriers include lack of insurance and limited access to culturally competent care. Women who engage in sex work and use drugs face unique challenges including competing survival needs, low risk perception, and difficulty with daily adherence. Effective strategies include nonjudgmental care provider communication, integrated HIV and substance use care, and adherence support. Clinicians may struggle with limited infrastructure and discomfort discussing sex work Harris, et al. 2024. Young MSM of color face care provider bias and a lack of culturally concordant care. Hiring staff with shared identities, providing affirming services, and LGBTQ+ cultural competency training can improve PrEP engagement Ribas Rietti Souto, et al. 2024. Individuals who inject drugs have low to moderate levels of PrEP awareness and very low PrEP uptake, varying from 0% to 3% in a systematic review Mistler, et al. 2021. There has been little research into effective ways to increase PrEP uptake in people who inject drugs. Addressing structural and stigma-related barriers for this population is essential. One study found that conversations about HIV prevention at syringe-exchange programs significantly increased PrEP awareness Walters, et al. 2020.
Despite increased availability of oral PrEP (tenofovir disoproxil fumarate/emtricitabine [TDF/FTC] or tenofovir alafenamide/emtricitabine (TAF/FTCJoseph Davey, et al. 2025. Expanding the number of PrEP prescribers beyond HIV and sexual health specialists to include primary care providers is essential. Additionally, clinicians must address unconscious bias, avoid assumptions about sexual or drug use behavior, and gain comfort with taking sexual histories Calabrese, et al. 2018; Edelman, et al. 2017; Calabrese, et al. 2014. If a patient requests PrEP and it is not medically contraindicated, it should be prescribed with appropriate follow-up.
Successful PrEP programs will address stigma, mistrust, low HIV risk perception, and structural inequities through culturally responsive, patient-centered care and offer flexible PrEP options, including the ability to switch modalities.
PrEP persistence and episodic use: PrEP effectiveness depends on sustained use, yet discontinuation remains common. A meta-analysis of oral PrEP use found that 41% of users discontinued within 6 months and 35.6% between 7 and 12 months, with discontinuation strongly associated with increased HIV incidence (2.1–3.6 vs. 0.0–0.1 per 100 person-years) Guo, et al. 2024. Discontinuation is more likely among younger people, individuals using substances (especially methamphetamine), women, and those with lower education or high out-of-pocket costs. Medicaid coverage, affordability, and living in an Ending the HIV Epidemic (EHE) county are associated with improved persistence Dawit, et al. 2024. Public transportation reliance is associated with lower continuation Sharpe, et al. 2023, while use of health-system specialty pharmacies (HSSPs) improves persistence at 6, 12, and 18 months Whelchel, et al. 2023.
Frequent required visits and laboratory testing can be experienced as “overmedicalization” and deter continuation. Although quarterly laboratory monitoring is standard for oral PrEP, it is not evidence-based and should be adapted to patient needs. At-home HIV testing or conveniently located external laboratory centers with annual in-person visits and telemedicine options can reduce structural barriers Siegler, et al. 2019.
PrEP use may be noncontinuous, with individuals cycling on and off based on perceived HIV risk. Discontinuation does not always reflect program failure Reed, et al. 2021. For individuals who wish to stay on PrEP, removing barriers and tailoring care are essential.
PrEP choice: Offering individuals a choice of HIV prevention modalities including oral PrEP, long-acting injectable PrEP, and post-exposure prophylaxis (PEP) improves uptake, adherence, persistence, and satisfaction. In the SEARCH trial, a dynamic choice model allowing participants to switch modalities led to more than 5-fold higher biomedical coverage (69.7% vs. 13.3%) and reduced HIV incidence (0% vs. 1.8%) compared with standard of care Kamya, et al. 2024. A modeling analysis projected that structured choice, including the option of CAB LA, could reduce HIV incidence by one-third over 10 years and be cost-effective across eastern and southern Africa Phillips, et al. 2025. In the ImPrEP CAB Brasil study, 83% of participants opted for CAB LA over oral PrEP after receiving options counseling, citing challenges with daily pills and confidence in injectables Grinsztejn, et al. 2025. PrEP options counseling significantly increased CAB LA uptake and satisfaction, highlighting the importance of decision-support tools in personalized HIV prevention. The approval of SC LEN adds another important PrEP choice and may further increase uptake and persistence.
Gender-affirming care and PrEP: Transgender women experience a disproportionate burden of HIV, and PrEP uptake is likely to have a high impact in transgender women who are sexually active and for whom PrEP is indicated Malone, et al. 2021. Transgender women have low rates of PrEP uptake and high rates of discontinuation Scott, et al. 2019, and gender-affirming care and access to hormone therapy can increase PrEP uptake and adherence Sevelius, et al. 2016. Gender-affirming care has been shown to improve health outcomes for transgender people, and providing gender-affirming hormone therapy in the context of primary care was associated with reduced rates of HIV seropositivity in the LEGACY study Reisner, et al. 2025. Concerns about interactions between PrEP medications and estrogen may lead to avoidance or missed doses, although studies show that TDF/FTC, TAF/FTC, CAB LA, and SC LEN do not significantly affect hormone levels Kelley, et al. 2025; Blumenthal, et al. 2022; Grant, et al. 2021; Blair, et al. 2020; Hiransuthikul, et al. 2019. Providing reassurance about this lack of interaction can also increase uptake.
Comprehensive services and support: To enhance PrEP success, it is essential that clinicians collaborate with others inside and outside their organizations to address individuals’ social determinants of health and offer services such as:
- Mental health and substance use treatment
- Case management and navigation
- Housing assistance and benefits counseling
- Support groups and peer networks
| KEY POINTS |
|
PrEP Coverage
Coverage under the Affordable Care Act (ACA): In 2023, the U.S. Preventive Services Task Force published an updated grade A recommendation that clinicians should “prescribe preexposure prophylaxis using effective antiretroviral therapy to persons at increased risk of HIV acquisition to decrease the risk of acquiring HIV” USPSTF 2023. This federal recommendation recognizes PrEP as a preventive service to be covered under the ACA, a significant step toward increasing access to PrEP, and further affirms PrEP as a highly effective HIV prevention strategy clinicians can and should provide to their patients. Of note, ACA plans and Medicare Part B and D not only cover PrEP medications but also testing and monitoring without cost-sharing CMS 2024.
Coverage in New York State: New York State Senate Bill S825 (2023-2024 Legislative Session) mandates that certain large group policies cover HIV PrEP and PEP. New York State Medicaid and the Essential Plan cover PrEP medications, visits, monitoring, and testing without cost-sharing (see NYS Medicaid Coverage for HIV PrEP Related Services).
| RESOURCES |
|
FDA-Approved PrEP Agents
Tenofovir disoproxil fumarate 300 mg/emtricitabine 200 mg in a fixed-dose tablet (TDF/FTC; Truvada): TDF/FTC is approved by the U.S. Food and Drug Administration (FDA) for use as PrEP as part of a comprehensive HIV prevention strategy for all individuals at risk of acquiring HIV. Multiple randomized, placebo-controlled clinical trials have demonstrated the efficacy of TDF/FTC as PrEP for preventing HIV infection in all risk populations when taken daily as directed McCormack, et al. 2016; Choopanya, et al. 2013; Baeten, et al. 2012; Grant, et al. 2010. Based on 2 large clinical trials, TDF/FTC can also be taken before and after sex (on-demand dosing) for appropriate candidates (see guideline section Choosing and Prescribing a PrEP Regimen > Alternative Oral Dosing: On-Demand PrEP), although this dosing strategy is not FDA-approved.
Tenofovir alafenamide 25 mg/emtricitabine 200 mg in a fixed-dose tablet (TAF/FTC; Descovy): TAF/FTC was noninferior to TDF/FTC in a study of men who have sex with men (MSM) and a small number of transgender women who have sex with men Mayer, et al. 2020. Daily TAF/FTC was approved by the FDA in October 2019 for HIV prevention through sexual exposure in those groups FDA(b) 2025. On-demand dosing of TAF/FTC has not been studied.
In the PURPOSE 1 trial, rates of HIV seroconversion with TAF/FTC were not different from the background rates of HIV seroconversion in cisgender adolescent and adult women overall Bekker, et al. 2024. However, in a subanalysis of the study TAF/FTC was effective when taken with medium to high adherence and reduced HIV incidence by 89% with 2 or more doses per week Kiweewa, et al. 2025. Although TAF/FTC is not FDA-approved for receptive vaginal sex, given the data noted above it is reasonable as part of shared decision-making to offer TAF/FTC as an alternative PrEP option for HIV exposures through receptive vaginal sex for individuals in whom TDF/FTC is not tolerated or not desired.
Long-acting injectable cabotegravir (CAB LA; Apretude): CAB LA is an integrase strand transfer inhibitor given as an intramuscular injection every 2 months after an optional 4-week lead-in of oral CAB (Vocabria) and 2 initial injections given 4 weeks apart. CAB LA was statistically superior to oral TDF/FTC as PrEP (due to imperfect adherence to oral PrEP) in MSM, transgender women, and cisgender women Delany-Moretlwe, et al. 2022; Landovitz, et al. 2021. CAB LA was approved by the FDA in December 2021 for prevention of HIV via all sexual exposures FDA 2021.
Subcutaneous lenacapavir (SC LEN; Yeztugo): SC LEN is a capsid inhibitor dosed subcutaneously every 6 months along with an initial oral loading dose of two 300 mg tablets on the day of the initial injections and again on the next day after the injections. In the PURPOSE 1 trial in cisgender adolescent and adult women Bekker, et al. 2024 and PURPOSE 2 trial in men and gender-diverse populations who have sex with men Kelley, et al. 2025, SC LEN was statistically superior to TDF/FTC (PURPOSE 1 and 2) and to TAF/FTC (PURPOSE 1) in preventing HIV infection for all sexual exposures (due to imperfect adherence to oral PrEP). The PURPOSE 3 (cisgender women in the United States), PURPOSE 4 (people who inject drugs), and PURPOSE 5 (individuals at high risk of HIV in France and the United Kingdom) trials are ongoing. SC LEN was approved by the FDA in June 2025 for prevention of HIV via all sexual exposures FDA(d) 2025.
Who Should Use PrEP
| RECOMMENDATIONS |
PrEP Candidates
Contraindications to PrEP
|
Abbreviations: ART, antiretroviral therapy; CrCl, creatinine clearance; nPEP, non-occupational post-exposure prophylaxis; PrEP, pre-exposure prophylaxis; TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC; tenofovir disoproxil fumarate/emtricitabine (Truvada). |
PrEP Candidates
PrEP is part of a comprehensive HIV prevention plan and should be offered to individuals, including adolescents who meet the prescribing criteria, and who are assessed as or who self-identify as being at increased risk of acquiring HIV through sexual or injection drug exposure.
| NEW YORK STATE LAW |
|
Box 1, below, shows candidates who should be offered PrEP and factors that do not disqualify candidates from PrEP. See Appendix B: Studies That Support the Use of PrEP in Different Populations for a discussion of the studies that support the use of PrEP in different populations.
| Box 1: Candidates for Pre-exposure Prophylaxis |
Offer pre-exposure prophylaxis (PrEP) to individuals who are candidates, including those who:
Do not withhold PrEP from eligible candidates who:
|
Contraindications to PrEP
Exposure to HIV in the previous 72 hours: Individuals with potential HIV exposure in the previous 72 hours should be prescribed PEP and provided a 4-week follow-up to transition to PrEP. See the NYSDOH AI guideline PEP to Prevent HIV Infection.
HIV infection: The 2-drug PrEP regimens of TDF/FTC and TAF/FTC and the single-drug regimens of long-acting injectable cabotegravir (CAB LA) and subcutaneous lenacapavir (SC LEN) are inadequate for treating established HIV infection; therefore, PrEP should not be initiated unless an individual is tested for HIV at initiation or within 1 week before the proposed initiation. If HIV infection is confirmed, PrEP should immediately be converted to a fully suppressive HIV treatment regimen. See guideline section Managing a Positive HIV Test Result.
Renal dysfunction: TDF is contraindicated for individuals with a CrCl <60 mL/min at the time of PrEP initiation and should be discontinued if CrCl drops to <50 mL/min FDA 2024. TAF/FTC can be prescribed in individuals with a CrCl ≥30 mL/min. Serum creatinine levels can vary and be affected by factors other than renal disease; therefore, before a decision is made to forgo or discontinue oral PrEP, decreased CrCl should be verified through repeat testing, and other causes of spurious creatinine elevation (e.g., use of creatine-containing protein supplements) or reversible causes (e.g., use of nonsteroidal anti-inflammatory drugs) should be ruled out. CAB LA and SC LEN are safe to use in individuals with renal dysfunction.
Fillers, implants, and silicone in the buttocks and hips: Caution should be exercised when considering CAB LA as PrEP in individuals with silicone and implants in buttocks and hips, as absorption of CAB LA may be compromised.
Drug-drug interactions: CAB LA as PrEP is contraindicated with some antiseizure medications and rifamycins. There are several important drug-drug interactions for SC LEN that require dose adjustment and consideration of alternative PrEP options. Check for drug-drug interactions before prescribing PrEP. See NYSDOH AI Drug-Drug Interaction Guide: From HIV Prevention to Treatment and University of Liverpool HIV Drug Interactions.
Other HIV prevention methods: Discuss other HIV prevention methods, such as condom use and safer sex practices, in the context of PrEP, particularly for individuals with contraindications or intolerance to current PrEP options.
Comparing PrEP Regimens
All current pre-exposure prophylaxis (PrEP) options are highly effective when taken as directed. Shared decision-making allows patient preferences and clinical considerations to guide the choice of the best PrEP option for each candidate (see Table 1 and Table 2, below).
| Abbreviations: 3TC, lamivudine; ART, antiretroviral therapy; CrCl, creatinine clearance; FDA, U.S. Food and Drug Administration; HBV, hepatitis B virus; IM, intramuscular; LDL, low-density lipoprotein; MSM, men who have sex with men; NYCRR, New York Codes, Rules and Regulations; PEP, post-exposure prophylaxis; PrEP, pre-exposure prophylaxis; TasP, treatment-as-prevention.
Notes:
|
||||
| Table 1: Key Clinical and Logistical Factors in Choosing a PrEP Regimen (details provided in discussion that follows; also see Checklist 1: Key Factors in Choice of PrEP Regimen) |
||||
| TDF/FTC (tenofovir disoproxil fumarate/emtricitabine; Truvada) |
TAF/FTC (tenofovir alafenamide/emtricitabine; Descovy) |
CAB LA (long-acting injectable cabotegravir; Apretude) |
SC LEN (long-acting injectable lenacapavir; Yeztugo) |
Comments |
| Indications | ||||
| Sexual and injection drug exposures use in adults and adolescents weighing ≥35 kg |
|
|
|
|
| Time to Protection [a] | ||||
|
Not defined, but expected to be ≤7 days | Estimated efficacy at 7 days | 2 hours after second oral loading dose | See guideline section Comparing PrEP Regimens > Time to Protection |
| Renal Safety | ||||
|
|
Increased monitoring for adverse effects is recommended if CrCl <30 mL/min. | Increased monitoring for adverse effects is recommended if CrCl <15 mL/min. | More frequent monitoring may be required for individuals at increased risk of renal disease (i.e., hypertension, diabetes, age >40 years). |
| Bone Safety | ||||
| Potential decrease in bone mineral density; meta-analysis shows good safety Pilkington, et al. 2018 |
|
Preferred option for prevention of sexual exposures in all individuals with osteopenia or osteoporosis | Preferred option for prevention of sexual exposures in all individuals with osteopenia or osteoporosis | — |
| Weight and LDL Cholesterol | ||||
|
|
|
No information on weight or cholesterol reported | — |
| Dosing | ||||
|
Daily dosing only |
|
|
— |
| Same-Day Initiation | ||||
| Generic TDF/FTC is a preferred insurance option and is usually available for same-day initiation. | May require prior insurance authorization |
|
|
— |
| Common Adverse Effects | ||||
| Diarrhea (6%), nausea (5%) Glidden, et al. 2016 | Diarrhea (5%), nausea (4%) Mayer, et al. 2020 | Injection site reactions (32% to 81%) Delany-Moretlwe, et al. 2022; Landovitz, et al. 2021, which are mostly mild and greatest initially | Injection site reactions including potential pain, nodules, and erythema (69% to 83%) Kelley, et al. 2025; Bekker, et al. 2024, mostly grades 1 and 2, affected by injection technique | — |
| Use During or When Planning Pregnancy | ||||
| May be continued through pregnancy and breast/chestfeeding | May be continued through pregnancy and breast/chestfeeding |
|
|
|
| Use With Oral Contraceptives | ||||
| No interaction expected based on pharmacokinetic data | No interaction expected based on pharmacokinetic data | No interaction expected based on pharmacokinetic data | May increase concentrations of oral contraceptives but no dose adjustment needed | No dose adjustment of emergency contraception needed for all PrEP regimens |
| Use With Gender-Affirming Hormones | ||||
| No significant interaction with estrogen or testosterone | No significant interaction with estrogen or testosterone | No significant interaction with estrogen or testosterone |
|
— |
| Patients With Active Chronic HBV [b,c] | ||||
|
Active against and FDA-approved for treatment of HBV infection | Not active against HBV infection | Not active against HBV infection | Monitor closely for rebound HBV viremia if TDF/FTC or TAF/FTC is discontinued in a patient with chronic HBV |
| Drug-Drug Interactions | ||||
| See NYSDOH AI Drug-Drug Interaction Guide: From HIV Prevention to Treatment > TDF and TAF Interactions | See NYSDOH AI Drug-Drug Interaction Guide: From Prevention to Treatment > TDF and TAF Interactions | See NYSDOH AI Drug-Drug Interaction Guide: From Prevention to Treatment > CAB Interactions | See NYSDOH AI Drug-Drug Interaction Guide: From Prevention to Treatment > LEN Interactions | Drug-drug interactions for SC LEN may require additional dosing or an alternative PrEP regimen. |
| Generic Formulation Availability | ||||
| Generic TDF/FTC is available | Brand only | Brand only | Brand only | TAF/FTC, CAB LA, and SC LEN may require prior insurance authorization. |
| Abbreviations: ART, antiretroviral therapy; CAB LA, long-acting injectable cabotegravir (Apretude); HBV, hepatitis B virus; HSV, herpes simplex virus; SC LEN, subcutaneous lenacapavir (Yeztugo) PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection; TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC, tenofovir disoproxil fumarate/emtricitabine (Truvada). | |||
| Table 2: Benefits, Limitations, and Risks of Available PrEP Regimens | |||
| All PrEP Regimens | Oral PrEP With TDF/FTC or TAF/FTC | Injectable PrEP With CAB LA | Injectable PrEP With SC LEN |
| Benefits | |||
|
|
|
|
| Limitations | |||
|
|
|
|
| Risks | |||
| Continued use after undiagnosed HIV infection may result in development of drug-resistant virus |
|
|
|
HBV Infection
Daily tenofovir-containing PrEP is preferred for individuals with chronic hepatitis B virus (HBV). Unlike tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) and tenofovir alafenamide/emtricitabine (TAF/FTC), long-acting injectable cabotegravir (CAB LA) and subcutaneous lenacapavir (SC LEN) do not prevent or treat HBV infection. When considering or switching to a long-acting injectable PrEP regimen, perform HBV testing if an individual’s hepatitis serologies are unknown or if there was borderline or low-level immunity in the past. Unrecognized chronic HBV can flare when tenofovir-containing regimens are discontinued. Individuals with chronic HBV who are switching from an oral PrEP regimen will need to continue oral tenofovir or other HBV treatment options while using CAB LA or SC LEN. Non–HBV-immune individuals should be offered routine vaccination to prevent HBV infection. See the NYSDOH AI guideline Prevention and Management of Hepatitis B Virus Infection in Adults With HIV.
Time to Protection
The time to protection against HIV infection after PrEP initiation is not definitively established. Whether the key to protection is drug levels in genital and rectal tissue, plasma blood mononuclear cells (PBMCs), or more likely, a combination of tissue and PBMC levels is under debate. Most of what is known is from animal studies, human tissue studies, and pharmacokinetic modeling. There are no studies with clinical endpoints. In animal models and observational studies, post-exposure prophylaxis (PEP) has been effective if initiated within 72 hours after exposure, which raises questions about the specific drug concentrations in tissue required to protect against HIV infection.
TDF/FTC: Early pharmacokinetic modeling data demonstrated that 7 days of daily TDF/FTC for PrEP are required to achieve maximal protective concentrations in rectal tissue, and 20 days of daily dosing are required to achieve maximal protective concentrations in cervicovaginal tissue Louissaint, et al. 2013; Anderson, et al. 2012; Patterson, et al. 2011. Newer pharmacokinetic modeling data suggest that TDF/FTC is likely protective within 1 week of dosing in both rectal and genital compartments and PBMCs Hendrix, et al. 2016; Seifert, et al. 2016. Emtricitabine triphosphate (active metabolite of emtricitabine) reaches steady-state and therapeutic concentrations very quickly in vaginal tissue, and tenofovir diphosphate (active metabolite of tenofovir) reaches concentrations more slowly, potentially affording vaginal protection quite early from emtricitabine triphosphate while tenofovir diphosphate concentrations accumulate Cottrell, et al. 2016; Seifert, et al. 2016.
Studies have shown that initiating PrEP with a double dose (2 tablets) of TDF/FTC confers protective levels after 2 hours both rectally and vaginally Chawki, et al. 2024; Cottrell, et al. 2016. Therefore, a double dose of TDF/FTC at initiation, when more immediate protection is desired, is recommended, otherwise daily dosing for 7 days will achieve optimal protective levels of medication in PBMCs and genital and rectal tissue, acknowledging that protection is likely conferred earlier.
TAF/FTC: Time to protection for TAF/FTC is also unclear. TAF had a faster time to 90% effective concentrations (EC90) than TDF (4 hours vs. 3 days) and significantly higher steady-state concentrations in PBMCs than TDF/FTC as PrEP Ogbuagu, et al. 2021, which may confer a clinical benefit in terms of time to protection and adherence forgiveness, but this is preliminary evidence and further evaluation is needed. It is reasonable to assume protection at 7 days, and likely earlier. There are no data on a double dose at initiation for more immediate protection.
CAB LA: CAB LA is estimated to be protective 7 days after the initial injection Han(a), et al. 2024. If switching from oral PrEP, individuals should be advised to continue oral PrEP for an additional 7 days to maintain protection while CAB LA levels are rising, otherwise counsel individuals on additional HIV prevention techniques, including barrier protection and abstinence, during this time.
SC LEN: Rapid increases have been observed in plasma concentrations of LEN after the initial oral loading dose and first injection, reaching therapeutic levels within 2 hours after the second oral loading dose on day 2 Gilead 2025; Jogiraju, et al. 2025, and it is reasonable to assume protection at that point. Individuals initiating SC LEN who are not already using PrEP should be counseled on using additional HIV prevention techniques, including barrier protection and abstinence, during the oral loading period. Individuals switching from oral PrEP to SC LEN are protected from HIV on the day of the initial injection. If the second oral loading dose is missed, the time to protection increases to up to 28 days Gilead 2025.
| KEY POINTS |
|
Choosing and Prescribing a PrEP Regimen
| RECOMMENDATIONS |
Choice of Regimen
TDF/FTC
TAF/FTC
Patients With HBV
CAB LA
SC LEN
|
Resources: Checklist 1: Key Factors in Choice of PrEP Regimen; Checklist 2: Assessment and Counseling Before PrEP Initiation Abbreviations: CAB LA, long-acting injectable cabotegravir (Apretude); CrCl, creatinine clearance; HBV, hepatitis B virus; IM, intramuscular; INSTI, integrase strand transfer inhibitor; MSM, men who have sex with men; oral CAB, oral cabotegravir (Vocabria); PrEP, pre-exposure prophylaxis; SC LEN, subcutaneous lenacapavir (Yeztugo); TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC, tenofovir disoproxil fumarate/emtricitabine (Truvada). |
Preferred Oral Regimen for Daily Dosing: TDF/FTC
TDF/FTC is the preferred oral HIV PrEP regimen because of its proven efficacy and safety in clinical trials, suitability for use in all populations, including individuals who inject drugs, and cost, which is significantly lower than that of TAF/FTC. However, for adults with preexisting renal disease or osteoporosis and for adolescents aged 19 years or younger, TAF/FTC is the preferred oral regimen (see discussion below).
Daily dosing: The U.S. Food and Drug Administration (FDA)-approved dosing of TDF/FTC as PrEP is 1 tablet daily by mouth with or without food FDA 2024.
Common adverse effects: In clinical trials of TDF/FTC as PrEP, the most common adverse effects were nausea, headache, abdominal pain, and dizziness, which were mild and short-lived McCormack, et al. 2016; Thigpen, et al. 2012; Grant, et al. 2010. Most adverse effects peaked at 1 month and generally resolved within 3 months Glidden, et al. 2016. In a study comparing TAF/FTC and TDF/FTC as PrEP, both regimens were well tolerated, with diarrhea the only treatment-related adverse effect in >10% of individuals in either study arm Mayer, et al. 2020.
Renal impairment and loss of bone density: Both renal impairment and loss of bone density have been observed in individuals taking TDF/FTC as HIV treatment, predominantly in studies of TDF/FTC combined with a third drug containing the pharmacokinetic booster ritonavir or cobicistat. Studies comparing unboosted TDF/FTC and TAF/FTC for HIV treatment found no difference in adverse events between the 2 regimens Hill, et al. 2018. A meta-analysis of 13 trials of TDF/FTC used as PrEP found no difference in serious adverse events between TDF/FTC and placebo but did find a borderline statistically significant difference in creatinine elevation of all grades when adding in grade 1 and 2 elevations Pilkington, et al. 2018.
The DISCOVER study, which compared TDF/FTC with TAF/FTC as PrEP, found a small but statistically significant difference between biomarkers of renal and bone dysfunction favoring TAF/FTC, although no difference was found in clinical adverse outcomes Mayer, et al. 2020. Although renal dysfunction is uncommon in individuals taking TDF/FTC as PrEP, and especially those who are younger than 50 years Gandhi, et al. 2016, regular laboratory monitoring is necessary during use of TDF/FTC or TAF/FTC (see Table 4: Recommended Routine Laboratory Testing for Individuals Using PrEP). If an increase in serum creatinine or a decrease in calculated CrCl is observed, evaluate potential causes other than TDF use. Discontinuation or interruption of TDF/FTC as PrEP is appropriate if other causes are ruled out or if CrCl drops to <50 mL/min (confirmed on 2 readings) for any reason. TAF/FTC is indicated for sexual exposures when CrCl ≥30 mL/min. When appropriate, on-demand dosing of TDF/FTC can also be considered to decrease drug exposure for individuals with borderline renal function.
Bone density losses with TDF/FTC as PrEP are minimal, have not been associated with bone fractures, and are reversible in individuals aged 20 years and older Havens, et al. 2020; Spinelli, et al. 2019. However, bone loss did not completely reverse in individuals aged 19 years and younger Havens, et al. 2020; therefore, TDF/FTC is not the preferred option in this age group (see Appendix B: Studies That Support the Use of PrEP in Different Populations > Adolescents > Oral PrEP).
Alternative Oral Regimen for Daily Dosing: TAF/FTC
TAF/FTC is an alternative oral HIV PrEP regimen for all sexual exposures. However, it is the preferred oral regimen (for all sexual exposures) for individuals with preexisting renal disease or osteoporosis and for individuals aged 19 years and younger. TAF/FTC may also be preferable when there are multiple risk factors for renal disease or osteoporosis.
Daily dosing: The FDA-approved dosing of TAF/FTC as PrEP is 1 tablet daily by mouth with or without food FDA(b) 2025. On-demand dosing has not been studied for TAF/FTC.
TAF/FTC for receptive vaginal exposure: Based on the PURPOSE 1 trial results showing 89% lower rates of HIV acquisition in cisgender women who took 2 or more doses per week Kiweewa, et al. 2025, use of TAF/FTC is appropriate for receptive vaginal sex in those whom TDF/FTC is not appropriate, tolerated or desired.
Common adverse effects: As noted above, in a study comparing TAF/FTC and TDF/FTC as PrEP, both regimens were well tolerated, with diarrhea the only adverse effect in >10% of individuals in either arm Mayer, et al. 2020.
Managing Adverse Effects of Oral PrEP
Two weeks after oral PrEP initiation, follow up with the individual either in person or by telephone to assess and address adverse effects and offer advice for management until they abate. Gastrointestinal adverse effects can be alleviated by taking PrEP medications with food or antidiarrheal agents, anti-gas medications, and antiemetics. In the iPrEx and Partners trials of TDF/FTC as PrEP, rash was not reported as a common adverse effect Mujugira, et al. 2016; Grant, et al. 2014; Grant, et al. 2010. Assess individuals who develop a rash while taking TDF/FTC or TAF/FTC as PrEP for syphilis and acute HIV Apoola, et al. 2002.
Alternative Oral Dosing: On-Demand PrEP
On-demand (also called intermittent or event-driven) PrEP, taking medication before and after sex instead of daily, is not FDA-approved, but strong evidence for the efficacy of on-demand dosing in cisgender MSM is based on results of the IPERGAY and Prevenir studies.
Background: The IPERGAY and Prevenir studies found that 2-1-1 dosing effectively prevented HIV acquisition in MSM Molina, et al. 2022; Molina, et al. 2015. Successful on-demand PrEP requires planning ahead for sex by at least 2 hours. Data on daily dosing of TDF/FTC are more robust than for on-demand dosing, with longer follow-up. However, the preferred dosing strategy is that which fits best into the individual’s lifestyle. Clinicians should review the individual’s usual sex planning practices and ensure they understand the complex on-demand dosing schedule. Switching between daily and on-demand PrEP as sexual activity changes is an appealing, evidence-based option for some individuals Molina, et al. 2022; Hoornenborg(b), et al. 2017. On-demand dosing of TDF/FTC is not recommended for blood exposures through injection drug use or in individuals with HBV.
Earlier studies have shown that estrogen use may lower tenofovir levels in the plasma of transgender women compared with cisgender men, but more recent studies call these findings into question (see Appendix B: Studies That Support the Use of PrEP in Different Populations > Transgender women). The PREVENIR and IPERGAY studies included too few transgender women who have sex with men to prove effectiveness in this population Molina, et al. 2022; Molina, et al. 2015. However, the lack of drug interactions with gender-affirming hormone therapy supports the use of on-demand PrEP in transgender women.
There are no studies of on-demand PrEP for receptive vaginal sex. Modeling data suggest that although tenofovir levels are lower in the female genital tract than in rectal tissue, FTC levels are high enough to offer significant protection at the tissue level within 2 hours of dosing. Tenofovir levels decrease in the female genital tract faster than in rectal tissues, but the addition of 1 more day of TDF/FTC increases protection from 85% to an estimated 93% to 98% Engel, et al. 2025. Systemic drug levels of TDF/FTC measured in PBMCs reflect intracellular concentrations necessary to inhibit HIV replication, regardless of tissue concentrations in the female genital tract. If individuals who are at risk of HIV exposure through receptive vaginal sex prefer an on-demand option instead of daily oral or injectable PrEP, it is reasonable to engage them in shared decision-making about on-demand PrEP (with an additional day of dosing) while awaiting clinical trial data.
Dosing strategies:
- On-demand dosing for rectal and penile exposures: TDF/FTC is taken as a “2-1-1” regimen:
- 2 to 24 hours before sex: Take 2 TDF/FTC tablets (closer to 24 hours is preferred), followed by
- 24 hours after sex: Take 1 TDF/FTC tablet, then
- 48 hours after sex: Take 1 TDF/FTC tablet
- If sex occurs again: Take 1 TDF/FTC tablet daily until 48 hours after the last sex act, effectively becoming daily PrEP for as long as sex continues.
- On-demand dosing for receptive vaginal exposures: TDF/FTC is taken as a “2-1-1-1” regimen:
- 2 to 24 hours before sex: Take 2 TDF/FTC tablets (closer to 24 hours is preferred), followed by
- 24 hours after sex: Take 1 TDF/FTC tablet, then
- 48 hours after sex: Take 1 TDF/FTC tablet
- 72 hours after sex: Take 1 TDF/FTC tablet
- If sex occurs again: Take 1 TDF/FTC tablet daily until 72 hours after the last sex act, effectively becoming daily PrEP for as long as sex continues.
- On-demand dosing cannot be recommended for protection against blood exposures.
There are no data to guide decisions on the use of on-demand PrEP for neovaginal or neopenile HIV exposures.
| KEY POINTS |
|
Injectable Regimen: CAB LA Every 2 Months
When CAB LA is preferred: Because of its statistically superior efficacy to oral PrEP regimens and its protection against HIV through all types of sexual exposure, CAB LA is a preferred PrEP agent for all adults and adolescents weighing ≥35 kg who are open to injectable PrEP. CAB LA is an advantageous option when oral medication poses a challenge to PrEP use. TDF/FTC (or TAF/FTC if available same day) can be used as an alternative therapy for same-day initiation when oral CAB or CAB LA is not immediately available because of insurance or logistics issues. Overlapping 7 days of oral TDF/FTC or TAF/FTC with CAB initiation can be used to maintain protection against HIV while CAB levels are attaining steady-state.
Oral CAB lead-in: In clinical trials of CAB LA, a 5-week oral CAB lead-in was administered to rule out adverse effects before individuals received a long-acting injection Delany-Moretlwe, et al. 2022; Landovitz, et al. 2021. Although there are no data on the safety or efficacy of CAB LA when used for PrEP without an oral lead-in, in clinical trials of long-acting injectable CAB plus rilpivirine (CAB/RPV LA) for HIV treatment, omission of the oral lead-in was safe and did not interfere with achievement of adequate plasma CAB levels when injections were initiated Orkin, et al. 2021. There were no CAB safety concerns identified during the oral lead-in phase in trials of CAB/RPV LA as HIV treatment Rizzardini, et al. 2020 or in trials of CAB LA as PrEP Delany-Moretlwe, et al. 2022; Landovitz, et al. 2021. As a result, the oral lead-in phase for CAB LA as PrEP is now optional.
Some care providers or individuals initiating PrEP who are concerned about tolerability may prefer an oral CAB lead-in. An important consideration in such cases is the potential risk of HIV acquisition for individuals who may struggle with adherence to daily oral medication. Of note, 3 of the 12 incident HIV infections in individuals using CAB as PrEP in the HPTN 083 study were acquired during the oral lead-in phase Marzinke(a), et al. 2021. Ongoing daily oral CAB is not FDA-approved or recommended as PrEP.
CAB LA injections: See Box 2, below, for details on the dosing, preparation, and administration of CAB LA as PrEP.
| Box 2: Dosing, Preparation, and Administration of Long-Acting Injectable Cabotegravir as Pre-Exposure Prophylaxis [a] |
Initiation and continuation doses:
Preparation and administration:
|
|
Note: |
Adverse effects: In the clinical trials noted above, CAB LA as PrEP was well tolerated. Adverse reactions observed in at least 1% of participants included injection site reactions, diarrhea, headache, pyrexia, fatigue, sleep disorders, nausea, dizziness, flatulence, abdominal pain, vomiting, myalgias, rash, decreased appetite, somnolence, back pain, and upper respiratory tract infection; however, almost all were grade 1–level effects Delany-Moretlwe, et al. 2022; Landovitz, et al. 2021. The most common adverse effects were injection site reactions in 81% of HPTN 083 study participants and 32% of HPTN 084 study participants. Reactions were mostly mild or moderate in intensity and decreased in frequency and intensity over time. Median onset was 1 day after injection in the HPTN 083 trial and lasted a median of 3 days. Discontinuations due to injection site reactions were rare and occurred at a rate of 2.4% in the HPTN 083 trial and 0.0% in the HPTN 084 trial. Other studies have reported a strong preference for long-acting injectable medications despite injection site reactions Tolley, et al. 2020; Murray, et al. 2018.
Drug-drug interactions: Strong inducers of cytochrome 450 (CYP), uridine diphosphate glucuronosyltransferase (UGT)1A and P-glycoprotein (P-gp) can significantly decrease CAB levels. Although the risk of drug-drug interactions when combining CAB LA with most medications used in primary care is low, there is a risk of reduced CAB drug concentrations when used concurrently with certain antiseizure drugs such as carbamazepine, oxcarbazepine, phenobarbital (and primidone), phenytoin, as well as with rifamycins. For guidance in managing CAB LA drug-drug interactions, consult the following resources:
- NYSDOH AI Drug-Drug Interaction Guide: From HIV Prevention to Treatment
- University of Liverpool HIV Drug Interactions
Metabolic effects: Mild weight gain was observed in MSM and transgender women receiving CAB LA as PrEP compared with TDF/FTC, but there was no significant difference in weight between the 2 study arms in cisgender women, and there was no significant effect on lipid levels Delany-Moretlwe, et al. 2022; Landovitz, et al. 2021.
Oral CAB as bridge therapy: Oral CAB can be used as bridge therapy when it is anticipated that a CAB LA injection will be missed. Oral CAB is currently only available from a central pharmacy in collaboration with ViiV Healthcare. TDF/FTC (or TAF/FTC if appropriate) can also be used as bridge therapy when logistics impede timely access to oral CAB.
Alternative sites of injection: Data on alternative sites of injection are insufficient. Thigh injections into the vastus lateralis muscle were associated with a 10% decrease in bioavailability and more rapid decline in drug levels Han(b), et al. 2024.
Managing missed injections: As mentioned above, CAB LA is given every 2 months, with a window period of 1 week before or after the prior injection. Missed injections are bridged with oral PrEP.
- Planned missed injection (>5 weeks since initiation injection or >9 weeks since last continuation injection): If an individual misses their CAB LA injection for a planned reason, initiate oral PrEP (oral CAB, TDF/FTC, or TAF/FTC) beginning when the injection is due and continuing until CAB LA can be administered. If it has been more than 12 weeks since their last injection, the individual can stay on oral PrEP or restart CAB LA injections with the 4-week loading dose.
- Unplanned missed injections: If an individual misses their CAB LA for an unplanned reason, determine why the individual is unable to return and refer them for appropriate services as needed. Offer the individual oral PrEP until injections can be resumed (if appropriate) and guidance as noted above for planned missed injections.
Discontinuing CAB LA: CAB levels begin to decline in the body 2 months after the last injection but persist and slowly decline over a median of 43.7 weeks for men and 67.3 weeks for women Landovitz, et al. 2020. During this time there are increasingly lower CAB levels that will not protect from HIV infection. Educate individuals receiving CAB LA as PrEP on the medication “tail” and provide individualized guidance on alternative PrEP options and prevention planning if HIV risk continues. If risk is ongoing, oral PrEP should be continued for at least 1 year to prevent the acquisition of INSTI-resistant HIV. However, it is reassuring that none of the individuals in the HPTN 083 study who acquired HIV during the tail phase had INSTI resistance-associated mutations Landovitz, et al. 2021.
Diagnosing HIV in individuals receiving CAB LA: Diagnosing HIV seroconversion in individuals receiving CAB LA can be challenging. For discussion of long-acting early viral inhibition (LEVI) syndrome with potential delayed HIV positivity, altered presentation of acute HIV, and altered testing algorithms while using CAB LA as PrEP, see guideline section Managing a Positive HIV Test Result > Ambiguous HIV Test Results > LEVI syndrome.
Injectable Regimen: SC LEN Every 6 Months
When SC LEN is preferred: Because of its statistically superior efficacy to oral PrEP regimens and its protection against HIV through all types of sexual exposure, SC LEN is a preferred PrEP agent for all adults and adolescents weighing ≥35 kg who are open to injectable PrEP.
Dosing: See Box 3, below, for details on the dosing, preparation, and administration of SC LEN as PrEP.
| Box 3: Dosing, Preparation, and Administration of Subcutaneous Lenacapavir as Pre-Exposure Prophylaxis [a] |
How supplied:
Initiation dose:
Continuation dose:
Preparation and administration:
|
|
Note: |
Adverse effects: The most common and expected adverse effects associated with SC LEN are injection site reactions (ISRs), which may include pain, erythema, swelling, nodules, induration, and pruritus. Individuals receiving SC LEN as PrEP should be counseled to expect potential discomfort, induration, and subcutaneous nodules in the first week after the injection. SC LEN injections commonly create persistent subcutaneous nodules, which in the PURPOSE-2 study lasted a median of 183 days Kelley, et al. 2025. Although they are generally painless, the nodules can be palpated and sometimes visible depending on the physique of the individual. ISRs rarely led to discontinuation Kelley, et al. 2025; Bekker, et al. 2024. Proper injection technique (using ice packs at the site before injection and injecting at a 90° angle) can significantly decrease the incidence and intensity of ISRs FDA(d) 2025; Kelley, et al. 2025.
Where to inject: The FDA label lists the preferred site of administration as the abdomen, with the thigh an accepted alternate site. However, pharmacokinetic data show similar or higher LEN levels for upper arm and thigh injections Lat, et al. 2023 and safety data show similar or lower rates of ISRs with thigh, upper arm, and gluteal region injections Saunders, et al. 2024, compared with abdomen injections. These data support using alternate injection sites based on patient preference.
Drug-drug interactions: Because LEN is a substrate and moderate inhibitor of CYP3A4 and a substrate of P-gp, the potential for drug-drug interactions associated with the use of SC LEN as PrEP should be carefully considered. Although the risk of drug-drug interactions when combining LEN with most medications used in primary care is low, there is a risk of reduced LEN drug concentrations when used concurrently with CYP3A4 or P-gp inducers. Examples of common CYP3A4 inducers can be remembered with the mnemonic COPPER: Carbamazepine, Oxcarbazepine, Phenobarbital (and primidone), Phenytoin, Enzalutamide, and Rifampin (also rifabutin and rifapentine). Although not a complete list, these are the most common CYP3A4 inducers used in clinical practice.
LEN increases drug concentrations of gamma-hydroxybutyrate (GHB), ketamine, benzodiazepines, fentanyl, and nitazenes, making adverse effects and overdose of these drugs when used concurrently with SC LEN a concern. LEN also increases drug concentrations of PDE5 inhibitors, which are used to treat erectile dysfunction. Taking amyl nitrates (“poppers”) with PDE5 inhibitors is contraindicated because of the risk of a severe drop in blood pressure, which would be more likely with concomitant SC LEN use. It is important that clinicians discuss the risk of and effects of drug-drug interactions with individuals receiving SC LEN.
Dosing of SC LEN with concomitant strong or moderate CYP3A4 inducers: Current FDA prescribing information for SC LEN for HIV prevention provides recommendations for supplemental dosing with LEN injections and/or oral tablets to offset potential interactions; these recommendations vary depending on whether a strong or a moderate CYP3A4 inducer is being added to LEN. For guidance in determining the degree of induction from CYP3A4 (and other isoenzymes of CYP450) when managing drug-drug interactions, consult the following resources:
- NYSDOH AI Drug-Drug Interaction Guide: From HIV Prevention to Treatment
- FDA Drug Development and Drug Interactions, Table of Substrates, Inhibitors and Inducers (may not contain all medications identified as CYP3A4 inducers)
- U.S. Department of Health and Human Services Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents With HIV > Drug-Drug Interactions
- University of Liverpool HIV Drug Interactions
Note that FDA recommendations for managing concurrent use of CYP3A4 inducers differ greatly in the prescribing information for LEN used as HIV prevention (Yeztugo) and LEN used for HIV treatment (Sunlenca).
| KEY POINTS |
|
Managing missed injections: As mentioned above, SC LEN is given every 6 months, with a window period of 2 weeks before or after the prior injection. Missed injections are bridged with oral LEN or another oral PrEP regimen if oral LEN is not available. For both planned and unplanned missed injections, if oral LEN is not initiated for bridging and more than 28 weeks have lapsed since the prior injection, reinitiation with oral LEN 600 mg daily for 2 days is needed in addition to LEN injections.
- Planned missed injection >14 days late (>28 weeks since the last injection): If an individual misses their LEN injection for a planned reason, initiate oral LEN 300 mg once every 7 days (beginning when the injection is due) and continue until SC LEN can be administered, up to a maximum of 6 months (26 weeks). If the injection is missed beyond 6 months (i.e., more than 52 weeks since the last injection), transition the individual to another PrEP regimen if they plan to continue PrEP (see Discontinuing SC LEN, below). If oral LEN is unavailable for bridging, prescribe another oral PrEP regimen.
- Unplanned missed injection >14 days late (>28 weeks since the last injection): If an individual misses their SC LEN injection for an unplanned reason, determine why the individual is unable to return and refer them for appropriate services as needed. Offer the individual oral LEN or another oral PrEP regimen as noted above for planned missed injections.
Discontinuing SC LEN: Levels of SC LEN begin to decline in the body 6 months after the last injection and continue to decline over the following 6 months (the medication “tail”). During this time there are increasingly lower levels of SC LEN that will not protect from HIV infection. Individuals receiving SC LEN as PrEP should be educated on the medication “tail” and provided individualized guidance on alternative PrEP options and prevention planning if HIV risk continues.
Managing a positive HIV test result: See guideline section Managing a Positive HIV Test Result. In the 2 seroconversions seen in the PURPOSE 2 study, no delay was observed in HIV antigen/antibody positivity, and viral load results were 14,100 and 934,000 copies/mL, respectively Kelley, et al. 2025. For individuals who have a positive HIV test result while receiving SC LEN as PrEP, an initial INSTI-based antiretroviral therapy (ART) regimen should be initiated (see the NYSDOH AI guideline Selecting an Initial ART Regimen).
| KEY POINT |
|
PrEP During Pregnancy
PrEP should be offered to pregnant individuals with ongoing HIV exposure, as HIV acquisition risk is higher during pregnancy and highest in the late pregnancy and early postpartum periods Thomson, et al. 2018. Risk of perinatal transmission is also significantly higher during pregnancy and breast/chestfeeding in cases of acute seroconversion Drake, et al. 2014; Singh, et al. 2012, and this committee recommends PrEP in individuals at risk while they are breast/chestfeeding. Encourage pregnant individuals to inform their obstetric and pediatric care providers when using PrEP medications or any other prescription or over-the-counter medications. Prospectively report pregnancies in individuals on PrEP to the Antiretroviral Pregnancy Registry.
TDF/FTC: TDF/FTC is considered safe to use during pregnancy FDA 2024. Available data suggest that TDF/FTC as PrEP does not increase the risk of congenital anomalies. Conflicting results have been observed in studies of bone mineral density in infants born to women taking TDF as a component of ART for HIV Siberry, et al. 2015; Vigano, et al. 2011. However, more recent studies of infants exposed to TDF in utero, 1 due to maternal HIV Reddy, et al. 2024 and 2 for HBV transmission prevention Wen, et al. 2020; Salvadori, et al. 2019, showed comparable bone mineral composition in exposed versus unexposed infants aged 1 to 7 years.
Infant exposure to TDF/FTC through breast milk is much lower than TDF exposure in utero; evidence to date suggests that TDF is safe during breastfeeding Liotta, et al. 2016; Ehrhardt, et al. 2015. Although data on breastfeeding effects are limited, TDF/FTC is commonly prescribed as part of an ART regimen before, during, and after pregnancy, and the benefit of preventing HIV infection and subsequent perinatal transmission among individuals at increased risk outweighs the theoretical concerns associated with prescribing TDF/FTC as PrEP during breastfeeding, pending further data.
TAF/FTC: Clinical trials, observational studies, and data from the Antiretroviral Pregnancy Registry support the use of TAF/FTC in pregnancy Zeng, et al. 2025. Further, the Society for Maternal-Fetal Medicine states that TAF/FTC has a similar safety profile to TDF/FTC for PrEP Badell, et al. 2024. TAF/FTC has been shown to be well tolerated and there have been no increased adverse pregnancy or infant outcomes in those taking TDF as PrEP or treatment for chronic HBV infection during pregnancy Heffron, et al. 2018.
CAB LA: No significant differences in maternal adverse events or pregnancy outcomes were observed between CAB LA and TDF/FTC in the HPTN 084 trial Delany-Moretlwe, et al. 2025. HPTN 084 researchers presented updated pharmacokinetic data for CAB LA as PrEP used before and during pregnancy. CAB LA was generally well tolerated. CAB LA levels declined in each trimester of pregnancy but remained above specific target levels. These findings suggest that no dose changes are needed when using CAB LA during pregnancy, although more human data are needed. None of the women who became pregnant while receiving CAB LA acquired HIV during their pregnancy. Use of CAB LA as PrEP appears to be safe during pregnancy, but data are limited. Use shared decision-making when considering whether to initiate or switch from CAB LA as PrEP for individuals who are pregnant or planning to conceive.
SC LEN: In the PURPOSE 1 study, there were 208 pregnancies and 132 live births in the SC LEN group, there were no pregnancy complications found to be related to SC LEN use, and the infant mortality rate was similar to background rates in the study region and to tenofovir-based PrEP FDA(d) 2025; Bekker, et al. 2024. No adverse effects related to SC LEN during breast/chestfeeding have been observed. Discuss potential risks and benefits and engage individuals who are or may become pregnant in shared decision-making when considering SC LEN as PrEP.
Initiating PrEP
| RECOMMENDATIONS |
Preinitiation Assessment
Baseline Laboratory Testing
Same-Day Initiation
Initiating PrEP During the HIV Testing Window Following Exposure
|
Resources: Checklist 2: Assessment and Counseling Before PrEP Initiation; Checklist 4: PrEP Initiation Abbreviations: Ag/Ab, antigen/antibody; ART, antiretroviral therapy; CAB LA, long-acting injectable cabotegravir (Apretude); CEI, Clinical Education Initiative; PEP, post-exposure prophylaxis; PrEP, pre-exposure prophylaxis. |
Before Initiating PrEP
Assess for acute HIV infection: Before initiating PrEP, all individuals should be evaluated for potential HIV exposure in the prior 6 weeks and assessed for the flu-like symptoms of acute HIV. Both an HIV-1/2 Ag/Ab combination immunoassay and an HIV RNA test should be performed within 1 week before PrEP initiation. HIV RNA (viral load) testing is recommended at baseline to rule out acute HIV infection regardless of reported risk, as individuals may be reluctant to disclose a recent potential risk exposure. If a confirmed negative result is not available at the time of the patient’s initial visit, a rapid HIV-1/2 test should be performed for same-day PrEP initiation.
Drug-resistant virus has been found in individuals with undiagnosed HIV who initiated PrEP with tenofovir disoproxil fumarate/emtricitabine (TDF/FTC), tenofovir alafenamide/emtricitabine (TAF/FTC), CAB LA and subcutaneous lenacapavir (SC LEN) Kelley, et al. 2025; Molina, et al. 2022; Landovitz, et al. 2021; Cox, et al. 2020; Lehman, et al. 2015.
Perform recommended laboratory testing: Table 3, below, lists the baseline laboratory tests that should be performed before PrEP initiation. When an individual is engaged in PrEP care, primary healthcare may also be offered as indicated, including vaccinations against hepatitis A and B viruses, human papillomavirus, meningococcus, mpox, influenza, and COVID-19 (see the NYSDOH AI guidelines Primary Care for Adults With HIV and Immunizations for Adults With HIV).
| Abbreviations: Ab, antibody; Ag, antigen; anti-HBc, hepatitis B core antibody; anti-HBs, hepatitis B surface antibody; CAB LA, long-acting injectable cabotegravir (Apretude); CDC, Centers for Disease Control and Prevention; CrCl, creatinine clearance; HAV, hepatitis A virus; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HCV, hepatitis C virus; IgG, immunoglobulin G; SC LEN, subcutaneous lenacapavir (Yeztugo); MSM, men who have sex with men; NAAT, nucleic acid amplification test; TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC, tenofovir disoproxil fumarate/emtricitabine (Truvada); UCSF, University of California San Francisco.
Notes:
|
||
| Table 3: Recommended Laboratory Tests for All individuals Within 1 Week Before Initiating PrEP [a] | ||
| Purpose (rating) | Test | Comments |
| HIV status (A*) |
|
|
| Renal function (A*) | Serum creatinine and calculated CrCl |
|
| Pregnancy status (A3) | Pregnancy test for all individuals of childbearing potential |
|
| HBV infection status (A2†) | HBV serologies: HBsAg, anti-HBs, and anti-HBc (IgG or total) |
|
| Syphilis screening (A2†) | All individuals: Syphilis testing [d] | Screen for syphilis according to the laboratory’s testing algorithm. |
| Gonorrhea and chlamydia screening (A2†) |
|
|
| HCV infection status (A3) | HCV serology with reflex to RNA | Inform individuals with HCV about transmission risk and offer or refer for treatment [f]. |
| HAV infection status (good practice) | HAV serology for MSM and individuals at high risk of HAV infection [g] | Vaccinate nonimmune individuals. |
| Hepatic function (good practice) | Serum liver enzymes | Increased serum liver enzymes may indicate acute or chronic viral hepatitis infection and require further evaluation. |
| Assess for preexisting renal disease, proteinuria, and glycosuria (good practice) | Urinalysis | Only calculated CrCl is used to guide decisions regarding the use of TDF/FTC and TAF/FTC as PrEP based on renal function; however, baseline urinalysis abnormalities may indicate an increased risk of renal tenofovir toxicity. |
Assessment and Counseling Before PrEP Initiation
Engagement in primary care: PrEP is an integral part of sexual health and well-being. Developing an HIV prevention plan that includes PrEP is an opportunity to engage individuals in primary care. Clinicians can encourage age-appropriate health screenings, substance use screening and interventions, linkage to specialty services, and other health maintenance activities such as immunizations (see the NYSDOH AI guideline Immunizations for Adults With HIV). For additional information, see Centers for Disease Control and Prevention Recommended Adult Immunization Schedule for Ages 19 Years or Older, United States, 2025 and ACIP Recommendations: COVID-19 Vaccine and NYSDOH Health Advisory: NYSDOH Meningococcal Vaccine Recommendations for HIV-Infected Individuals and Those at High Risk of HIV Infection.
Patient education: Patient education is vital to shared decision-making and the success of PrEP as part of a comprehensive HIV prevention plan. Educate PrEP candidates about its risks and benefits and the choice of oral versus injectable PrEP. Discuss individual preferences, needs, and circumstances. Adherence and persistence improve when individuals participate in medication-related decisions and are informed about the strong efficacy of PrEP when taken as directed Grinsztejn, et al. 2025 (see guideline section Adherence, below). Education provided in the individual’s native or preferred language and tailored to the individual’s level of comprehension and health literacy will help ensure understanding of the benefits and potential adverse effects, the need for adherence, regular monitoring, the process of obtaining refills for oral PrEP, payment and payment assistance, and how safer sex or drug injection practices decrease the risk of pregnancy or of acquiring HIV and other sexually transmitted infections (STIs) (see Be in the KNOW > Sex and HIV and NYSDOH Syringe Access and Disposal).
Sex and drug use histories: A detailed HIV risk assessment includes obtaining a patient’s sexual history and drug use history and having a frank, open, and nonjudgmental discussion of risk-related behaviors. As indicated, this discussion may also include offering further counseling and referrals, such as for substance use treatment (see NYSDOH Office of Addiction Services and Supports > Treatment and guidelines on Substance Use Care).
Viral load status of sex partner(s) with HIV: The antiretroviral therapy (ART) and viral load status of a sex partner with HIV may inform the discussion of risk. Sexual transmission of HIV does not occur when an individual with HIV has a persistently undetectable HIV viral load; nonetheless, an individual without HIV in a serodifferent partnership who does not have HIV may still elect to use PrEP Rodger, et al. 2016 (see discussion below). If the patient’s partner has detectable virus and genotypic test results are unavailable, knowledge of the partner’s ART regimen may be helpful. HIV acquisition risk is increased when an individual is exposed to HIV that is resistant to the components of their PrEP regimen Gibas, et al. 2019; Knox, et al. 2017. The potential for drug resistance is an important consideration when choosing a PrEP regimen. If there is a risk for drug resistance in a sex partner with HIV, choose a PrEP option to which said partner is not known to be resistant.
HIV-serodifferent couples: As mentioned above, in an HIV-serodifferent partnership the partner who does not have HIV may decide to use PrEP even if the partner with HIV has achieved an undetectable viral load with ART. Although this supplemental protection is likely unnecessary in light of the finding that undetectable = untransmittable (U=U), PrEP can be discussed as an additional option for HIV prevention. The partner without HIV may choose to take PrEP for other reasons, including if they have additional sex partners, are unsure of a sex partner’s viral load or ability to maintain viral suppression, or feel more secure about and in control of their sexual health with the added protection of PrEP. In September 2017, the NYSDOH endorsed the U=U consensus statement from the Prevention Access Campaign. For more information, see Appendix B: Studies That Support the Use of PrEP in Different Populations > HIV-serodifferent couples and NYSDOH AI U=U Guidance for Implementation in Clinical Settings.
Reproductive counseling: Inquire about the individual’s reproductive plans and provide preconception counseling when indicated. Determine whether they or their partner is pregnant or breast/chestfeeding, intends to conceive, or is currently using hormonal or other contraception in addition to condoms Bujan and Pasquier 2016; Lampe, et al. 2011; Vernazza, et al. 2011. Counsel HIV-serodifferent couples who are considering the use of PrEP during attempts to conceive about the utility, safety, and possible risks of the medication (see guideline section Choosing and Prescribing a PrEP Regimen > PrEP During Pregnancy).
Psychosocial assessment: Assessments of psychosocial needs, strengths, challenges, mental health, and substance use are integral to good general medical practice. In the case of someone prescribed PrEP, such assessments enable clinicians to identify modifiable barriers to adherence and provide services and referrals to support adherence and retention in care.
PrEP after PEP: Individuals who remain at increased risk of HIV exposure after completing a course of non-occupational post-exposure prophylaxis (nPEP) and are negative for HIV at the 4-week test should be offered PrEP to begin immediately after the last dose of nPEP. Giving a prescription for the first month of PrEP at the time PEP is prescribed can significantly increase access to and uptake of PrEP Cockbain, et al. 2022.
| KEY POINTS |
|
Same-Day PrEP Initiation
Once laboratory specimens are obtained (see Table 3, above) PrEP may be initiated while test results are pending as long as results will be available and addressed within 7 days and a rapid HIV test result is negative and if the individual has not had symptoms or signs of acute HIV in the prior 6 weeks, has no history of renal disease, and no risk exposures in the past 72 hours requiring PEP. Same-day PrEP initiation has been shown to be safe, and delayed PrEP initiation has been associated with a significant rate of loss to follow-up Kamis, et al. 2019; Mikati, et al. 2019. Same-day PrEP initiation may engage individuals more fully in care and reduce HIV exposures while test results are pending and encourages immediate attention to insurance coverage for PrEP or identification of other options for payment if needed.
Same-day PrEP initiation also risks starting a nonsuppressive ART regimen in someone with HIV. However, if laboratory results are available promptly, the PrEP regimen for an individual who tests positive for HIV can be intensified to a fully suppressive ART regimen and a referral for HIV care can be made. If the baseline HIV testing result is positive after the individual has received the first CAB LA injection, the clinician should consult with an experienced HIV care provider regarding the best way to intensify the PrEP regimen to a fully suppressive ART regimen (see guideline section Managing a Positive HIV Test Result). If a patient has a positive HIV test result after receiving the first dose of SC LEN, they should be placed on any preferred regimen as per HIV treatment guidelines.
TAF/FTC may require a prior authorization, which can make same-day initiation a challenge, but generic TDF/FTC is usually available for same-day initiation. If prior insurance authorization is required, same-day CAB initiation (oral or injection) and SC LEN may not be possible. Implementation challenges such as stocking and storing injectable medications in advance may also be prohibitive. If same-day initiation of CAB LA or SC LEN is not possible, an oral PrEP regimen can be an interim option while barriers to accessing injectable PrEP are addressed.
Although delays such as insurance barriers may impede PrEP initiation, the overall goal should be same-day initiation in individuals without renal disease, need for PEP, or signs or symptoms of acute HIV.
Initiating PrEP during the HIV testing window period: The window period is the time between when an individual has acquired HIV and when a diagnostic test can detect infection. The median time to positivity is 12 days for an HIV viral load test and 18 days for a laboratory-based HIV-1/2 Ag/Ab combination immunoassay; however, the 99th percentile for a positive test is 33 days for an HIV viral load test and 42 days for a laboratory-based HIV-1/2 Ag/Ab combination immunoassay Delaney, et al. 2017. Clinicians should not defer initiation of PrEP in candidates who, based on their reported sexual and drug use exposures, may be in the window period for seroconversion; doing so risks additional exposures and significant delays in PrEP initiation. Repeat HIV testing 1 month after PrEP initiation to help identify potentially positive individuals in a timely manner (see guideline section Ongoing Laboratory Testing).
| KEY POINTS |
|
Adherence
Challenges: Adherence remains a critical factor for oral PrEP effectiveness and is difficult for some individuals because of a range of intersecting factors, including pill size, tolerability, privacy concerns, PrEP-related stigma, neurocognitive impairment, mental health conditions, substance use, history of trauma, personal beliefs, travel, occupational demands, and health literacy. Although once-daily and on-demand oral PrEP dosing options are available, real-world experience and research continue to show adherence challenges for certain populations. Effective HIV prevention with TDF/FTC requires at least 4 doses per week Engel, et al. 2025; Grant, et al. 2014, and TAF/FTC effectiveness was found to be similar to TDF/FTC based on adherence Kiweewa, et al. 2025.
Timely injections are essential for long-acting injectable PrEP, as missed and delayed injections can cause viral breakthrough Landovitz, et al. 2021.
Strategies for adherence support: For oral PrEP, strategies to support and improve adherence include increasing visit frequency or follow-up contact, particularly for populations such as adolescents in whom adherence declined when visits shifted from monthly to quarterly Hosek, et al. 2017. Individualizing assessment of adherence barriers and incorporating peer support can also reinforce medication and appointment adherence Goodreau, et al. 2018; Jenness, et al. 2016.
For those unable or unwilling to maintain adherence to daily oral PrEP despite support efforts, long-acting injectable PrEP is an additional preferred PrEP option. Studies indicate strong interest in injectable PrEP among the general population and key subgroups Grinsztejn, et al. 2025; Philbin, et al. 2021; Koren, et al. 2020; Rael, et al. 2020. Injection appointment reminders and ongoing counseling on the importance of on-time injections are crucial to effective injectable PrEP programs.
If injectable PrEP is not desired or is not an option, alternative options should be considered, including on-demand PrEP or intermittent use (e.g., during periods of higher risk). If these options are not feasible, clinicians may consider discussing PrEP discontinuation alongside other HIV prevention strategies that align better with the patient’s needs and preferences.
| KEY POINTS |
|
Ongoing Laboratory Testing
| RECOMMENDATIONS |
Ongoing Laboratory Testing
HIV Testing
Renal Function Testing
STI Screening
HCV Screening
Pregnancy Screening
|
Resource: Checklist 5: PrEP Follow-Up Abbreviations: Ag/Ab, antigen/antibody; CrCl, creatinine clearance; FDA, U.S. Food and Drug Administration; HCV, hepatitis C virus; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection; TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC, tenofovir disoproxil fumarate/emtricitabine (Truvada). |
Services for follow-up and monitoring of individuals receiving PrEP are part of a comprehensive HIV prevention plan: routine HIV testing; risk-reduction counseling; access to condoms and syringes; STI, mental health, and substance use screening; and referral for treatment when indicated.
Table 4, below, lists the laboratory tests that should be performed for individuals using oral or injectable PrEP.
| Abbreviations: Ab, antibody; Ag, antigen; CAB LA, long-acting injectable cabotegravir (Apretude); CrCl, creatinine clearance; HCV, hepatitis C virus; SC LEN, subcutaneous lenacapavir (Yeztugo); oral CAB, oral cabotegravir (Vocabria); PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection; TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC, tenofovir disoproxil fumarate/emtricitabine (Truvada).
Notes:
|
|||
| Table 4: Recommended Routine Laboratory Testing for Individuals Using PrEP | |||
| Test | Laboratory Testing Indications | ||
| All PrEP Regimens | Oral PrEP: TDF/FTC or TAF/FTC |
Injectable PrEP: CAB LA or SC LEN |
|
| HIV-1/2 Ag/Ab combination immunoassay [a] |
|
|
|
| HIV RNA assay [a] | When a patient has symptoms of acute HIV [b] (A2) |
|
|
| Serum creatinine and calculated CrCl | — |
|
At least annually (A3) |
| STI (gonorrhea, chlamydia, and syphilis) screening (A2†) Note: Screening can be less frequent in those at lower risk |
Ask about symptoms at every visit; if present, perform diagnostic testing and treat as indicated | Every 3-6 months based on reported risk |
|
| HCV serology [d] | At least annually if at risk (A3) | — | — |
| Pregnancy test in individuals of childbearing potential |
|
— | — |
| Urinalysis | — | Annually (B3) | — |
HIV Testing
For individuals using PrEP, routine HIV testing is recommended for early detection of PrEP failure. None of the available regimens are adequate for treating acute or chronic HIV infection. Continued use of only TDF/FTC, TAF/FTC, long-acting injectable cabotegravir (CAB LA), or subcutaneous lenacapavir (SC LEN) in the presence of HIV infection may lead to viral resistance to these drugs.
Routine HIV testing with oral PrEP: A quarterly (every 3 months) HIV-1/2 Ag/Ab combination immunoassay is recommended for individuals taking TDF/FTC or TAF/FTC as PrEP. Quarterly HIV RNA testing is not needed for individuals who report consistent adherence to oral PrEP.
Breakthrough HIV infections among individuals adherent to oral PrEP are rare. When failure of an oral PrEP regimen occurs, it is usually associated with poor adherence and is infrequently associated with the development of resistance. When drug resistance develops, it is typically an M184V/I resistance mutation, which has little or no effect on subsequent response to HIV treatment. The development of the K65R resistance mutation (associated with tenofovir) has rarely been reported van de Vijver, et al. 2021; Gibas, et al. 2019. Unrecognized acute HIV infection at the time of PrEP initiation carries the highest risk for developing resistance mutations van de Vijver, et al. 2021; Gibas, et al. 2019. For this reason, this committee recommends that clinicians perform baseline HIV RNA testing for all individuals before initiating PrEP.
In the HPTN 083 study, there was less delay in detection of new HIV infections with seroconversion for participants receiving TDF/FTC than for those receiving CAB LA. There were a median of 34 days and 31 days of unrecognized baseline and incident HIV infections, respectively, in the TDF/FTC arm, compared with 62 days and 98 days, respectively, in the CAB LA arm Marzinke(a), et al. 2021.
HIV RNA testing is recommended for individuals who report an interruption in PrEP of more than 1 week or report missing doses of PrEP during a time of sexual activity since the preceding visit.
| KEY POINT |
|
Testing for HIV every 3 months is based on good practice rather than evidence. If HIV testing is missed, every effort should be made to avoid interruption of PrEP, as the potential harm of discontinuing PrEP outweighs the theoretical risk of delaying HIV testing in a stable individual. It is reasonable to provide an additional month of PrEP and plan for HIV testing as soon as possible.
In-office visits are not a requirement for ongoing prescription of PrEP. Individuals established on oral PrEP can be tested for HIV every 3 months, either on site or at an outside laboratory, and see their care providers every 6 to 12 months. Requiring in-office visits may create a barrier to PrEP access for some individuals. Alternative monitoring models, such as at-home testing and telehealth visits, can decrease barriers to PrEP access and monitoring.
Routine HIV testing with CAB LA: CAB LA injections are administered by clinic staff every 2 months. HIV Ag/Ab testing should be performed at the end of the oral CAB lead-in (if implemented) and at every injection visit. Breakthrough HIV infections were observed in 4 individuals who received on-time CAB LA injections in the HPTN 083 study, and were also observed during the oral CAB lead-in phase and during treatment interruptions Marzinke(a), et al. 2021. Adherence to the CAB LA injection schedule is not a guarantee of protection against HIV acquisition.
HIV RNA tests were initially recommended at all injection visits due to the long delay in HIV Ag/Ab conversion while on CAB LA PrEP (98 days for incident infections) Eshleman, et al. 2022; Marzinke(a), et al. 2021 (see guideline section Managing a Positive HIV Test Result > Ambiguous HIV Test Results > LEVI syndrome). However, when viral load tests were added to HIV Ag/Ab testing at all CAB LA injection visits in the HPTN 083 open-label extension study, there was a 75% rate of false-positive viral load test results, especially after 6 months of CAB LA use Landovitz(b), et al. 2024. Therefore, the use of routine viral load monitoring in individuals using CAB LA as PrEP is no longer recommended. In the HPTN 083 and 084 studies, false-positive viral load test results led to interruptions in PrEP use while negative results were confirmed.
Routine HIV testing with SC LEN: SC LEN injections are administered by clinic staff every 6 months. HIV Ag/Ab testing should be performed at the initial injection visit and every continuation injection visit. Two breakthrough infections with on-time injections were observed in the PURPOSE 2 study, 1 of which was found at an interim 3-month visit Kelley, et al. 2025. Adherence to the SC LEN injection schedule is not a guarantee of protection against HIV acquisition, and it is reasonable to perform interim 3-month HIV testing along with interim STI screenings for individuals at high risk. HIV RNA testing is not necessary after the initial injection visit unless there has been a delay in the injection schedule without oral bridging medication.
HIV testing if exposure is suspected: For individuals who present for PrEP initiation but have had a potential HIV exposure within the past 30 days, initial HIV testing may not detect early infection. Therefore, repeat HIV testing 1 month after initiation is recommended to rule out early HIV infection. For individuals who report an interruption in PrEP during a time of sexual activity, an HIV-1/2 Ag/Ab combination immunoassay and HIV RNA test are recommended when reinitiating PrEP.
HIV testing if acute HIV is suspected: Vigilance for signs and symptoms of potential HIV seroconversion in individuals using PrEP is crucial. If acute HIV is suspected, the clinician should perform an HIV-1/2 Ag/Ab combination immunoassay and a quantitative HIV RNA test Chin, et al. 2013; Apoola, et al. 2002. When testing for acute HIV infection is indicated, any use of a rapid HIV-1/2 Ag/Ab test should be followed with a laboratory-based HIV-1/2 Ag/Ab combination immunoassay. Detection of HIV RNA or Ag in the absence of serologic evidence of HIV should be considered a preliminary positive result (see guideline section Managing a Positive HIV Test Result).
For more detailed recommendations on testing for acute HIV, see the NYSDOH AI guidelines Diagnosis and Management of Acute HIV Infection and HIV Testing.
| KEY POINTS |
|
Routine Laboratory Testing
Renal function testing: One sign of tenofovir toxicity is the development of proteinuria and glucosuria. A baseline urinalysis along with serum creatinine levels help identify preexisting abnormalities before PrEP initiation. Periodic renal function monitoring is also important while a patient is taking TDF/FTC or TAF/FTC as PrEP. An elevated creatinine level should prompt an assessment for causes of renal dysfunction other than tenofovir, such as the use of nonsteroidal anti-inflammatory drugs, and an assessment for possible spurious elevation caused by use of creatine supplements.
After initiation of TDF/FTC or TAF/FTC as PrEP in adults younger than 40 years with no evidence of current or ongoing risks for renal dysfunction, creatinine screening can be done every 6 to 12 months. More frequent creatinine screening may be appropriate in individuals older than 40 years because renal toxicity is more likely to occur in this population Gandhi, et al. 2016. More frequent screening may also be appropriate for individuals with comorbidities, such as diabetes or hypertension, and those taking concomitant nephrotoxic drugs that might increase the risk of renal dysfunction.
CAB LA and SC LEN are not known to cause renal dysfunction, but caution and increased monitoring for adverse effects is recommended when CrCl is <30 mL/min for CAB LA and <15 mL/min for SC LEN. Baseline testing and annual monitoring of renal function are recommended.
STI screening: High baseline STI rates are seen among PrEP users. Starting PrEP offers a valuable entry point for routine STI screening and treatment, especially for asymptomatic infections. Relying solely on symptom-based screening misses many infections. Frequent testing allows early diagnosis and treatment, preventing complications such as neurosyphilis and pelvic inflammatory disease and reducing onward transmission Tang, et al. 2020; Golub, et al. 2016; Liu, et al. 2016. Modeling data indicate that wider PrEP use combined with regular STI screening and treatment reduces overall STI incidence even if condom use declines, by identifying and treating asymptomatic infections Jenness, et al. 2017. There is currently international debate as to whether the benefits of screening for asymptomatic gonorrhea and chlamydia in cisgender men and transgender women who exclusively have sex with men outweigh the risks, given the lack of significant long-term adverse outcomes from these infections in these populations. Treating asymptomatic gonorrhea and chlamydia have not driven down STI rates as expected, and there is increasing concern about rising antibiotic resistance Williams, et al. 2023. However, until there is further evidence and consensus on this subject, this committee continues to endorse routine screening.
Recommended testing and intervals: Testing intervals are set to align with visit frequency. See Table 4: Recommended Routine Laboratory Testing for Individuals Using PrEP, above.
Perform syphilis serologic testing routinely. Screen for gonorrhea and chlamydia based on reported sites of exposure, using nucleic acid amplification tests (NAATs) because of their higher sensitivity compared with culture. The FDA has approved diagnostic extragenital gonorrhea and chlamydia tests FDA 2019, making access to testing more readily available.
For men who have sex with men (MSM) and transgender women, default to 3-site testing (urethral/genital, rectal, and pharyngeal) unless declined, as extragenital infections are common and often missed by urine-only testing Pitasi, et al. 2019; Patton, et al. 2014. Studies have reported high rates of extragenital gonococcal and chlamydial infections in transgender men attending STI clinics Pitasi, et al. 2019; therefore, risk for extragenital STIs should be considered in this population. Vaginal swabs are preferred for cervical infections because of their higher sensitivity, urine samples are recommended for urethral infections because of comfort. For transgender women with a neovagina, data are lacking regarding optimal specimen type (neovaginal swab vs. urine-based testing). There are some reports of gonococcal infections detected via testing obtained from the neovagina van der Sluis, et al. 2015. Self-collected swabs for vaginal, rectal, and pharyngeal specimen types have performed well in many studies and are preferred by many individuals (see NYSDOH Sexually Transmitted Infection Self-Collection Outside of a Clinic Setting in New York State: Frequently Asked Questions) Dize, et al. 2016; Lunny, et al. 2015; Workowski and Bolan 2015; Taylor, et al. 2013.
Doxycycline post-exposure prophylaxis (doxy-PEP): Clinicians should offer doxy-PEP for STI prevention to cisgender MSM and transgender women who engage in condomless sex with partner(s) assigned male sex at birth, and who have had a bacterial STI diagnosed in the past year, or who have ongoing risk of STI exposure. See the NYSDOH AI guideline Doxycycline Post-Exposure Prophylaxis to Prevent Bacterial Sexually Transmitted Infections for more information. Doxy-PEP was not effective for receptive vaginal sex Stewart, et al. 2023, but the result may have been due to low adherence. Additional trials are underway to reassess use in this population. Clinicians should engage in shared decision-making with cisgender men who are at ongoing risk of STI exposure and engage in condomless sex with multiple partners assigned female sex at birth, offering doxy-PEP on a case-by-case basis.
| KEY POINTS |
|
Annual HCV screening: MSM, particularly those living with HIV, are at increased risk for acquiring HCV Fierer and Factor 2015; Bradshaw, et al. 2013 and data show elevated risk among MSM using PrEP as well Price, et al. 2019; Hoornenborg(b), et al. 2017. A case-control study identified risk factors for HCV acquisition in MSM with HIV, including recent ulcerative STIs, condomless receptive anal intercourse, sharing sex toys, unprotected fisting, injection drug use, and sharing straws for intranasal drug use Vanhommerig, et al. 2015. These behaviors may also elevate HCV risk in MSM without HIV and in the broader population. Annual HCV screening is recommended for MSM, transgender women who have sex with men, and individuals who inject drugs while using PrEP. More frequent testing should be considered for individuals at highest risk or with abnormal liver function test results.
Pregnancy screening: In individuals of childbearing potential using PrEP, routine assessment for the possibility of pregnancy and testing as appropriate can decrease potential concerns associated with unplanned pregnancies. Individuals of childbearing potential who are using PrEP and wish to avoid pregnancy should be offered contraception.
Managing a Positive HIV Test Result
| RECOMMENDATIONS |
Suspected Acute HIV
Reactive HIV Screening Test Result While Using PrEP
Ambiguous HIV Test Results
ART Selection for a Positive HIV Test Result or When Choosing to Intensify ART for an Ambiguous HIV Test Result
|
Abbreviations: Ag/Ab, antigen/antibody; APHL, Association of Public Health Laboratories; ART, antiretroviral therapy; CAB LA, long-acting injectable cabotegravir (Apretude); CDC, Centers for Disease Control and Prevention; CEI, Clinical Education Initiative; INSTI, integrase strand transfer inhibitor; PI, protease inhibitor; PrEP, pre-exposure prophylaxis; SC LEN, long-acting injectable lenacapavir (Yeztugo); TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC, tenofovir disoproxil fumarate/emtricitabine (Truvada). |
PrEP Failure
PrEP failure is rare, and HIV acquisition is almost always caused by lack of adherence to oral medication or injection schedules.
Oral PrEP: HIV acquisition while taking oral PrEP is related to suboptimal adherence in all but a small number of cases, and in most cases of acquisition while adherent to PrEP there was unrecognized HIV infection at the time of PrEP initiation. Other potential causes include exposure to resistant virus, exposure to an extremely high viral inoculum, or pharmacokinetic variability.
CAB LA: PrEP failures with CAB LA are rare. In studies, failure mainly occurs during the optional oral lead-in before the first injection, a missed or late injection, or during the tail phase after treatment discontinuation. In the HPTN 083 study, 6 individuals acquired HIV despite on-time CAB LA injections Landovitz, et al. 2022; Landovitz, et al. 2021. In at least 3 of these failures CAB LA was absorbed more quickly and/or levels declined more rapidly than the mean Marzinke, et al. 2023.
Integrase resistance mutations were found in 5 of 9 participants with a resistance test result in the HPTN 083 study Marzinke(a), et al. 2021. There were 4 PrEP failures with CAB LA in the HPTN 084 study, with 1 infection occurring in an individual who received on-time injections; no integrase resistance was found among these participants Marzinke(b), et al. 2021. With long-acting injectable medications there is concern about the slow decay in drug levels over time once the medication is stopped and that individuals who acquire HIV during the CAB LA tail phase might develop integrase resistance. It is reassuring that in the HPTN 083 study, none of the individuals who acquired HIV during the tail phase had integrase resistance mutations.
SC LEN: The PURPOSE 1 study had no PrEP failures in participants receiving SC LEN Bekker, et al. 2024. In the PURPOSE 2 study there were 2 seroconversions with capsid inhibitor resistance despite on-time injections Kelley, et al. 2025. The cause of these 2 PrEP failures is unclear and currently under investigation.
Suspected Acute HIV
Vigilance for signs and symptoms of potential HIV seroconversion in individuals receiving PrEP is crucial. TDF/FTC, TAF/FTC, CAB LA, or SC LEN as PrEP are inadequate treatments for acute or chronic HIV infection, and continued use in individuals with HIV may lead to the emergence of viral resistance to these drugs.
The mean time from HIV exposure to onset of symptoms in acute HIV infection is generally 2 to 4 weeks, with a range of 5 to 29 days; however, some individuals are asymptomatic and some have presented with symptoms up to 3 months after exposure Apoola, et al. 2002. This time course may be prolonged in individuals who acquire HIV while using PrEP, and symptoms of acute HIV infection may be blunted by TDF/FTC, TAF/FTC, SC LEN, and, particularly, CAB LA use (see Ambiguous HIV Test Results, below). While evaluating individuals for possible acute HIV infection, advise them to refrain from sexual activity or use condoms to minimize the risk of transmitting HIV to a partner without HIV.
For individuals with symptoms consistent with acute HIV infection who have a nonreactive HIV test result but have a plasma HIV RNA level ≥200 copies/mL, a clinician can make a presumptive diagnosis of acute HIV, perform HIV genotype testing, obtain routine initial HIV laboratory tests, and recommend immediate ART initiation.
For individuals who have a nonreactive HIV test result but have an HIV RNA level <200 copies/mL, clinicians should repeat HIV RNA testing and HIV diagnostic testing according to the standard HIV laboratory testing algorithm to exclude a false-positive test result versus a true-positive test result with a blunted viral response due to the use of antiretroviral drugs. Unless suspicion for acute HIV is low, initiate ART while seeking a definitive diagnosis.
Confirmed Reactive HIV Screening Test Result
A complete HIV treatment regimen should be initiated immediately upon confirmation of HIV infection while awaiting further test results, including resistance testing.
Oral PrEP: Because HIV acquisition in individuals taking oral PrEP is most often due to nonadherence, most HIV infections in these individuals are with wild-type virus (virus without resistance mutations). When resistance does occur, FTC-associated resistance due to the emergence of the M184V/I mutation is the usual finding, and tenofovir-associated resistance with the K65R mutation is rare Girometti, et al. 2022; Mayer, et al. 2020; Lehman, et al. 2015. Therefore, in individuals taking oral PrEP who have a positive HIV test result, it is reasonable to initiate a 3-drug INSTI-based ART regimen while awaiting resistance test results.
Injectable PrEP: For individuals who have a positive HIV test result while receiving CAB LA as PrEP, a PI-based ART regimen should be initiated while awaiting confirmation of HIV infection and resistance test results. If no INSTI resistance is found, the patient can be switched to an INSTI-based ART regimen if desired. For individuals who have a positive HIV test result while receiving SC LEN as PrEP, an INSTI-based ART regimen should be initiated while awaiting confirmatory test results. For more information, see the NYSDOH AI guidelines Rapid ART Initiation and Selecting an Initial ART Regimen.
Ambiguous HIV Test Results
Antiretroviral medications used as PrEP can blunt viral load response or cause an undetectable viral load and delay or change the antibody response to an acute infection. Interpreting HIV test results may be complicated by the effect of PrEP on viral and immune markers when the current CDC/APHL testing algorithm is followed Landovitz(a), et al. 2024; Zucker, et al. 2018; Hoornenborg(a), et al. 2017; Knox, et al. 2017; Markowitz, et al. 2017. If an HIV test result is indeterminate or ambiguous, a decision must be made as to the likelihood of the result being a false positive or a true positive with an altered timeframe or testing algorithm due to the use of antiretroviral medications as PrEP. Assessing adherence can assist with PrEP management while further testing or expert consultation is pending. Because HIV acquisition is rare in someone who is fully adherent to oral or injectable PrEP, a positive HIV test result is more likely to be a false positive in such an individual. There is an increased possibility of a true-positive test result when an individual reports gaps in adherence or access to oral PrEP medications, a delayed injection visit for injectable PrEP without oral bridging medication, or symptoms consistent with acute HIV since their last HIV test.
Oral PrEP: There are no commercially available tests of medication concentrations to confirm longer-term adherence to current oral PrEP regimen. Hair samples and dried blood spots are used in research only. Because false-positive HIV-1/2 Ag/Ab combination immunoassay results occur and there is a risk of HIV exposure if PrEP is discontinued, PrEP should be continued while awaiting confirmation. Clinicians should decide whether to continue PrEP or intensify to a fully suppressive ART regimen (see section above) while awaiting confirmatory test results, based on the degree of suspicion for a false-positive or true-positive HIV test result. Clinicians should perform supplemental diagnostic testing as soon as possible according to the standard HIV laboratory testing algorithm. Multiple tests over time may be needed. See A Strategy for PrEP Clinicians to Manage Ambiguous HIV Test Results During Follow-Up Visits for a thorough review of this topic Smith, et al. 2018.
CAB LA: There were several cases of HIV acquisition during the oral lead-in phase in clinical trials of CAB LA. If an individual has a positive HIV test during or shortly after taking oral CAB, assess for adherence and proceed as described above for oral PrEP. Assessing adherence to the CAB LA injection schedule is straightforward, and a true-positive result is more likely with delayed injections without oral bridging medication; however, there were 6 breakthrough HIV infections with CAB LA despite on-time injections in the HPTN 083 study Landovitz, et al. 2021. Interpreting HIV test results can be particularly challenging because of the propensity for CAB LA to affect symptoms and markers of acute HIV infection, leading to long-acting early viral inhibition (LEVI) syndrome.
LEVI syndrome: In the HPTN 083 study, a median delay of 98 days (range, 35-185 days) from HIV acquisition to a positive HIV Ag/Ab test result was observed in individuals receiving CAB LA as PrEP Marzinke(a), et al. 2021. LEVI syndrome is an altered presentation of acute HIV in individuals using CAB LA as PrEP, is characterized by low or undetectable HIV RNA and diminished or delayed Ab production, and is usually clinically silent Landovitz(a), et al. 2024. Because levels of HIV Ag, Ab, RNA, and DNA may be ambiguous and revert from reactive, indeterminate, or positive to nonreactive or negative, confirming HIV infection can be challenging. Confirmatory HIV assay results can remain negative or indeterminate as long as 1 year after HIV diagnosis. Expert consultation is advised to determine the best next steps when someone has an indeterminate HIV test result while using CAB LA as PrEP. Often, repeat testing over time is needed, and a decision should be made on whether to intensify to a fully active ART regimen while awaiting further testing.
SC LEN: In the 2 cases of seroconversion in the PURPOSE 2 study, a positive HIV Ag/Ab test result after HIV acquisition did not appear to be delayed Kelley, et al. 2025.
Management summary: In cases of ambiguous HIV test results in individuals using PrEP, repeating HIV testing in a few days may resolve ambiguity if the initial results were due to early infection or technical issues.
If ambiguity persists, continue PrEP, intensify to a full HIV treatment regimen while waiting for additional testing to resolve the ambiguity, or discontinue PrEP and allow viral replication to occur and be measured if the individual does have HIV. However, discontinuing PrEP leaves an individual who does not have HIV at risk, and delaying intensification risks loss of the theoretical virologic and immunologic benefits of early ART in an individual who does have HIV. Given the complexities of this issue, consultation with an experienced HIV care provider is recommended.
| KEY POINTS |
|
Discontinuing PrEP
| RECOMMENDATIONS |
Discontinuing PrEP
|
Abbreviations: CAB LA, long-acting injectable cabotegravir (Apretude); CrCl, creatinine clearance; HBV, hepatitis B virus; MSM, men who have sex with men; PrEP, pre-exposure prophylaxis; SC LEN, subcutaneous lenacapavir (Yeztugo); TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC, tenofovir disoproxil fumarate/emtricitabine (Truvada). |
The 2-drug PrEP regimens of TDF/FTC and TAF/FTC and the single-drug injectable regimens of CAB LA and SC LEN are inadequate for HIV treatment. If HIV infection is confirmed, PrEP should be converted immediately to a fully suppressive HIV treatment regimen (see guideline section Managing a Positive HIV Test Result).
Renal dysfunction: Monitor renal function as outlined in the guideline section Ongoing Laboratory Testing. If an increase in serum creatinine or a decrease in calculated CrCl is observed, evaluate potential causes other than TDF or TAF use, such as the use of nonsteroidal anti-inflammatory drugs (NSAIDs), spurious elevations due to creatine supplementation, or recent heavy exercise leading to muscle breakdown, and repeat testing to confirm the finding before considering discontinuation. TDF/FTC as PrEP should be discontinued in individuals who develop a confirmed CrCl <50 mL/min to avoid further toxicity. In 1 study, a majority of participants with a creatinine clearance of <60 mL/min were able to continue TDF/FTC after repeating laboratory testing, discontinuing oral protein supplements 2 days before laboratory testing, and/or addressing substance and NSAID use, and on-demand dosing did not lead to further deterioration of renal function Liegeon, et al. 2024.
On-demand TDF/FTC is a potential option for those with borderline renal function who do not have access to or interest in alternative PrEP options. Although TDF/FTC for HIV treatment can be adjusted to every-other-day dosing in individuals with a CrCl between 30 mL/min and 49 mL/min, this strategy has not been established for PrEP and should not be used. TAF/FTC is an option for individuals with CrCl ≥30 mL/min. CAB LA and SC LEN are options for all individuals with renal dysfunction who are at risk for HIV infection. Increased monitoring for adverse effects is recommended for those with severe or end-stage renal impairment.
Change in risk profile: Individuals may choose to discontinue PrEP when their risk for HIV acquisition is no longer a concern. If an individual decides to stop using PrEP because of the challenges of adhering to medication and visits but is still at risk for HIV acquisition, make attempts to individualize care to maintain access to the protection afforded by PrEP. Individuals who decide to discontinue PrEP and have a recent HIV exposure should continue PrEP until 48 hours after last rectal exposure and 72 hours after last vaginal receptive exposure, based on data regarding on-demand dosing. For individuals who do not adhere to the testing requirements for the safe prescribing of PrEP, PrEP should be discontinued only after repeated attempts have been made to accommodate specific patient needs and engage the patient in ongoing PrEP care.
HBV infection: Because discontinuation of TDF/FTC or TAF/FTC in individuals with chronic HBV infection can exacerbate HBV Buti, et al. 2015; Dore, et al. 2010; Chamorro, et al. 2005, an alternative treatment plan for these individuals is critical. For more information, see Centers for Disease Control and Prevention Recommendations for Routine Testing and Follow-up for Chronic HBV Infection.
Managing the pharmacokinetic tail of long-acting injectable drugs: Long-acting injectable drug levels decline after the last injection. Levels of CAB LA begin to decline 2 months after the last injection and continue for at least 1 year. Levels of SC LEN begin to decline 6 months after the last injection and decline over the next 6 months. During this time there are increasingly lower levels of these drugs as PrEP that will not protect from HIV infection and could potentially place the individual at risk of developing drug-resistant HIV if they were to seroconvert with subtherapeutic plasma levels. Individuals should be educated on the medication “tail” and provided individualized guidance on alternative PrEP options and prevention planning if HIV risk continues.
Planning for PrEP reinitiation: Individuals may discontinue PrEP for various reasons, including reduced exposure risk, adverse effects, and access challenges. When possible, clinicians should discuss the process of restarting PrEP at the time of discontinuation. Individuals that were taking oral PrEP may still have a supply of PrEP and it is important that these individuals understand how to restart, time to protection, and PrEP initiation laboratory testing requirements, including HIV testing (see guideline section Initiating PrEP).
| KEY POINTS |
|
Appendix A: Checklists for PrEP Regimen Choice, Assessment and Counseling, Implementation, Initiation, and Follow-Up
Checklist 1: Key Factors in Choice of PrEP Regimen
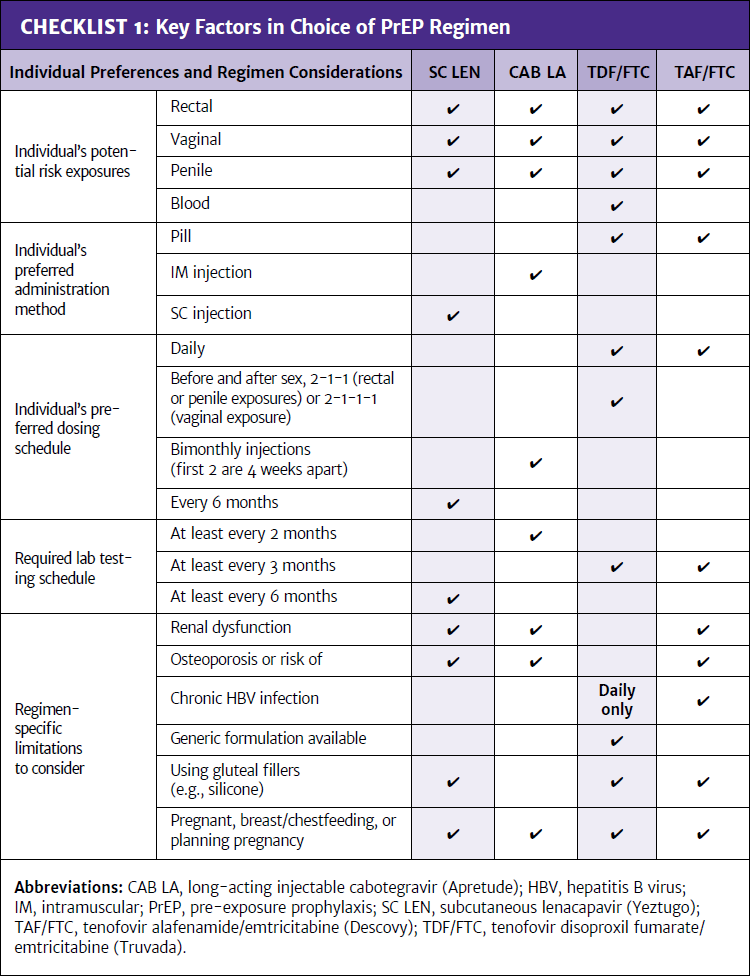
Checklist 2: Assessment and Counseling Before PrEP Initiation
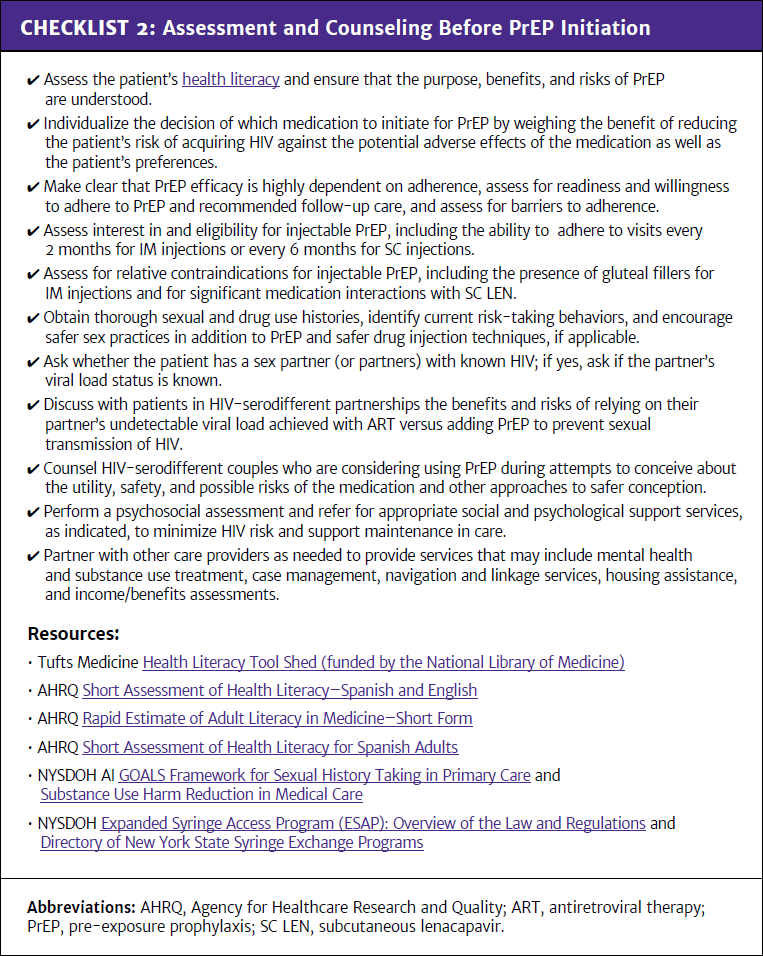
Checklist 3: Implementation Strategies for Long-Acting Injectable PrEP Regimens
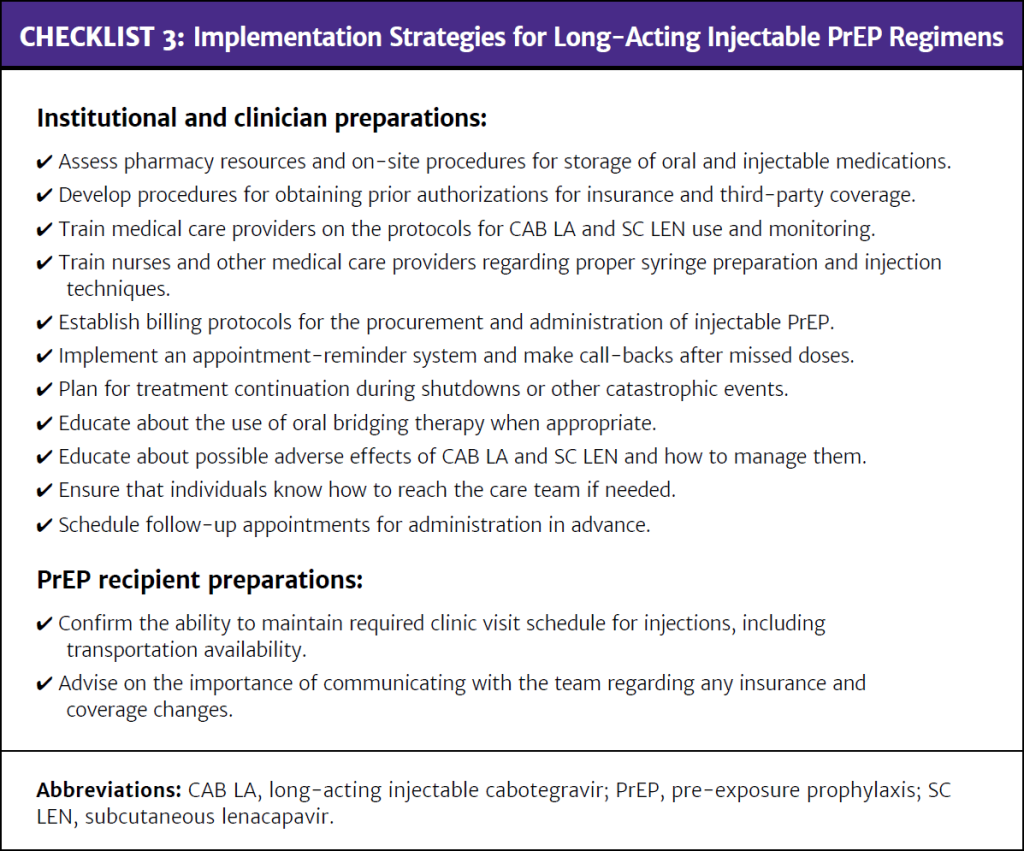
Checklist 4: PrEP Initiation
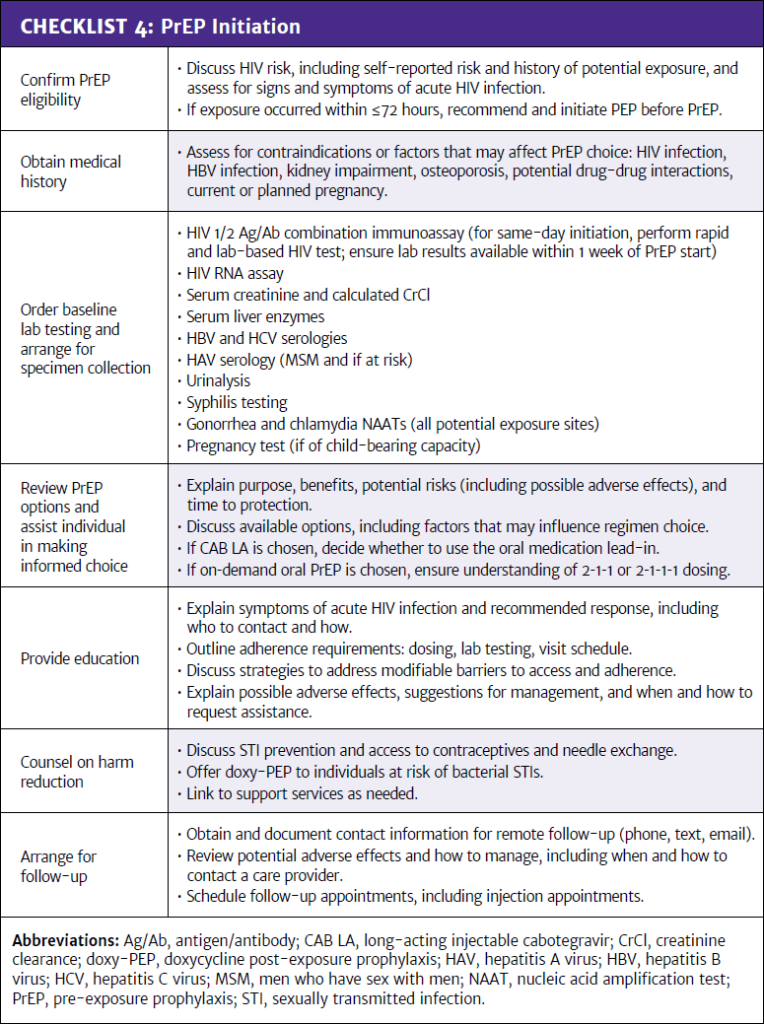
Checklist 5: PrEP Follow-Up
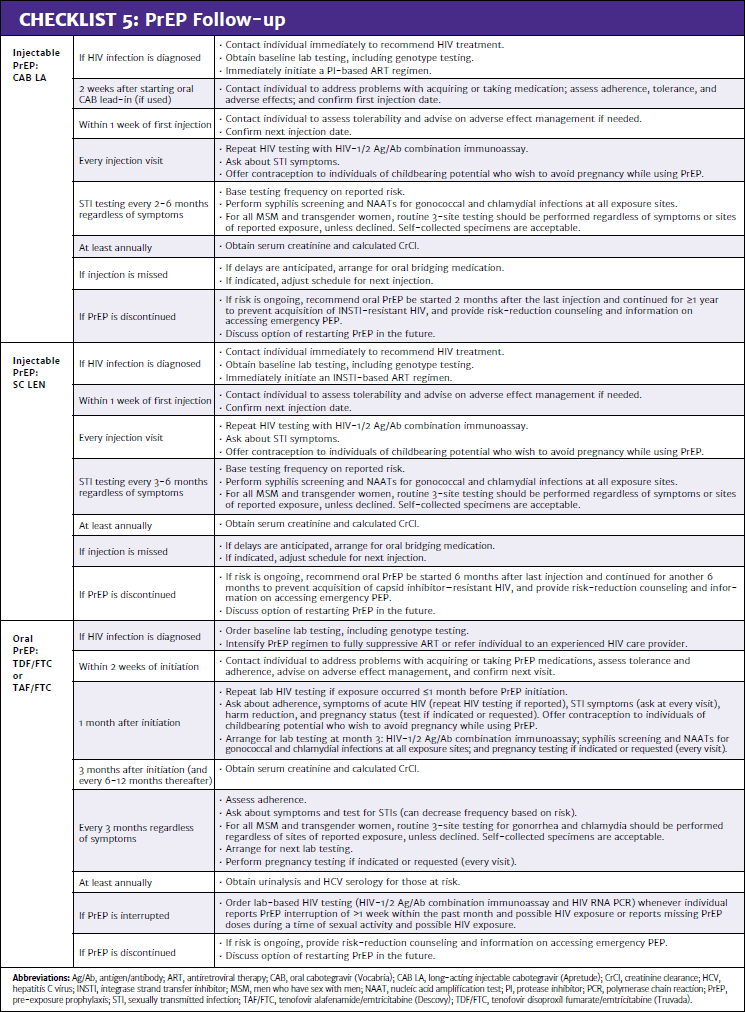
Appendix B: Studies That Support the Use of PrEP in Different Populations
Men who have sex with men (MSM):
- Studies have demonstrated that tenofovir disoproxil fumarate (TDF)/emtricitabine (FTC) as pre-exposure prophylaxis (PrEP) is highly effective in MSM Mayer, et al. 2020; McCormack, et al. 2016; Molina, et al. 2015; Grant, et al. 2014; Grant, et al. 2010.
- Although initial data from the iPrEx study demonstrated only a 44% reduction in the rate of HIV acquisition, there was a 92% reduction in sexual HIV transmission when tenofovir was detectable in the blood, and no seroconversions occurred in individuals with therapeutic plasma concentrations of TDF/FTC Grant, et al. 2010. Additionally, based on intracellular concentrations of tenofovir diphosphate, HIV risk-reduction was estimated to be 99% with 7 doses per week, and there were no seroconversions in individuals who took 4 or more doses per week Anderson, et al. 2012.
- In the PROUD study, TDF/FTC as PrEP had an overall efficacy rate of 86%, and there were no HIV infections in participants who took TDF/FTC as prescribed McCormack, et al. 2016.
- In the IPERGAY and the PREVENIR studies, on-demand or 2-1-1 dosing of TDF/FTC as PrEP was shown to be effective in cisgender men Molina, et al. 2022; Molina, et al. 2015.
- The DISCOVER study showed use of both TDF/FTC and tenofovir alafenamide (TAF)/FTC as PrEP to be highly effective in reducing the risk of HIV acquisition in MSM, with a combined total of 22 participants with new HIV infections in 8,756 person-years of follow-up; all except 2 were either infected at baseline or had low tenofovir plasma concentrations at the time of infection Mayer, et al. 2020.
- In the HPTN 083 study, both TDF/FTC and long-acting injectable cabotegravir (CAB LA) prevented HIV in MSM and transgender women; however, CAB LA was statistically superior, with 14 incident infections among participants receiving CAB LA, compared with 41 incident infections among participants taking TDF/FTC during the blinded phase of the study, mostly driven by poor adherence to TDF/FTC Landovitz, et al. 2022; Landovitz, et al. 2021.
- In the PURPOSE 2 trial, subcutaneous lenacapavir (SC LEN) was highly effective in preventing HIV in cisgender MSM, transgender women, transgender men, and nonbinary individuals; HIV acquisition was 0.10 per 100 person-years in the SC LEN group and 0.93 per 100 person-years in the TDF/FTC group, and HIV incidence with SC LEN was 96% lower than background (background HIV incidence was 2.37 per 100 person-years) Kelley, et al. 2025.
Transgender women:
- In the iPrEx study, TDF/FTC as PrEP was effective in transgender women who adhered to the regimen. Deutsch, et al. 2015.
- Multiple studies have shown that TDF/FTC does not alter estrogen levels Senneker 2024; Yager, et al. 2022; Grant, et al. 2021; Hiransuthikul, et al. 2019; Shieh, et al. 2019.
- Small studies have raised the possibility that estrogen lowers tenofovir levels by approximately 12% in the plasma of transgender women compared with cisgender men, or lowers levels of active metabolite in rectal tissues Cottrell, et al. 2019; Shieh, et al. 2019. However, in several subsequent studies, including the iBrEATHe and ImPrEPT studies, there were no significant interactions between hormone therapy and TDF/FTC Blumenthal, et al. 2022; Grant, et al. 2021.
- The PREVENIR and IPERGAY studies of on-demand PrEP with TDF/FTC included too few transgender women who have sex with men to prove effectiveness in this population Molina, et al. 2022; Molina, et al. 2015. However, the lack of drug interactions with gender affirming hormone therapy supports the use of on-demand PrEP in transgender women (see guideline section Preferred Oral Regimen for Daily or On-Demand Dosing: TDF/FTC).
- TAF/FTC was effective as PrEP in transgender women in the DISCOVER study, although transgender women made up only 1% of the study population Mayer, et al. 2020.
- Studies show that TAF does not alter estrogen levels and estrogen does not alter TAF levels Hiransuthikul, et al. 2025; Patel, et al. 2024.
- In the HPTN 083 study of CAB LA as PrEP, transgender women made up 12.5% of the study population and CAB LA was effective across all subpopulations Landovitz, et al. 2021. Additionally, oral CAB pharmacokinetics were not significantly altered by low-dose hormones used for oral contraceptives in the HPTN 077 study, and CAB LA does not alter estrogen levels Blair, et al. 2020.
- The PURPOSE 2 study showed SC LEN as PrEP to be highly effective and included a significant number of transgender women Kelley, et al. 2025.
Transgender men:
- Clinical trial data are lacking regarding the efficacy of TDF/FTC, TAF/FTC, and CAB LA as PrEP for transgender men who have sex with either cisgender men or transgender women, despite the increased risk of HIV acquisition in this population Pitasi, et al. 2019; Scheim, et al. 2017.
- TDF/FTC as PrEP is effective for all sexual exposures, including insertive vaginal sex and receptive anal sex, and is expected to be effective in transgender men.
- There was an 89% reduction in HIV risk among cisgender women who had at least 2 doses of TAF/FTC per week in the PURPOSE 1 trial; therefore, TAF/FTC is expected to be effective in transgender men Kiweewa, et al. 2025.
- In the iBrEATHe study, TDF/FTC did not lower testosterone levels in transgender men compared with controls, and testosterone did not lower tenofovir levels in transgender men compared with cisgender men Grant, et al. 2021.
- There are no relevant interactions between CAB and testosterone and no specific reason to suspect that CAB LA as HIV PrEP will be less effective for vaginal or anal exposures in transgender men FDA(c) 2025.
- The PURPOSE 2 study, which showed SC LEN to be highly effective in preventing HIV infection, was the first to intentionally include transgender men and gender-nonbinary individuals in their protocol Kelley, et al. 2025.
Cisgender men and women:
- Studies have demonstrated that TDF/FTC as PrEP is effective for cisgender men and women Baeten, et al. 2012; Thigpen, et al. 2012.
- In the Partners PrEP study of TDF/FTC, there was a 67% overall reduction in HIV acquisition in cisgender men and women and a 90% reduction among participants with detectable tenofovir in their blood Baeten, et al. 2012.
- In the TDF2 study, there was a 62% overall reduction in HIV acquisition, but there were only 2 seroconversions in participants who had detectable drug levels Thigpen, et al. 2012.
- The FEM-PrEP and VOICE trials did not demonstrate a benefit of TDF/FTC as PrEP for cisgender women; however, subsequent analyses found that this was due to poor adherence Van Damme, et al. 2012.
- TAF/FTC as PrEP was studied in cisgender adolescent and adult women as part of the PURPOSE 1 trial Bekker, et al. 2024. The incidence of new HIV infections among participants taking TAF/FTC or TDF/FTC were not different from background HIV rates, but adherence to both PrEP regimens was low. Participants with medium (4-6 doses per week) or high (7 doses per week) adherence to TAF/FTC had significantly lower odds of acquiring HIV infection than those with low adherence (odds ratio, 0.11).
- Cisgender women who took at least 2 doses of TAF/FTC per week in the PURPOSE 1 trial had an 89% reduction in HIV risk Kiweewa, et al. 2025, supporting the use of TAF/FTC in this population. In the same trial, SC LEN was 100% effective in preventing HIV infection.
- CAB LA was statistically superior to TDF/FTC as PrEP in the HPTN 084 study among cisgender women, in which there were 34 incident infections in the TDF/FTC arm but only 4 incident infections in the CAB LA arm, a difference driven by lower adherence to oral medication Delany-Moretlwe, et al. 2022.
HIV-serodifferent couples:
- Data from the HPTN 052 study demonstrated a reduction of 93% in HIV transmission risk in HIV-serodifferent heterosexual couples when the partner with HIV was on early versus delayed ART, and there were no phylogenetically linked transmissions at 5-year follow-up when partners were stably suppressed Cohen, et al. 2016.
- In the Partner Rodger, et al. 2016, Partner 2 Rodger, et al. 2019, and Opposites Attract Bavinton, et al. 2018 studies, there were no sexual transmissions between HIV-serodifferent partners when the partner with HIV had an undetectable viral load.
People who inject drugs:
- The Bangkok Tenofovir Study is the only randomized controlled trial of PrEP in people who inject drugs Choopanya, et al. 2013. PrEP efficacy with TDF alone, in this study, was 49%, although restricting analysis to participants with detectable TDF levels in their blood increased efficacy to 74%.
- The PURPOSE 4 trial is currently evaluating SC LEN for use in people who inject drugs.
- Given the pharmacokinetic levels of PrEP medications in peripheral blood mononuclear cell (PBMCs), it is reasonable to assume that all current PrEP options would be appropriate for use in people who inject drugs, excluding on-demand dosing.
Adolescents:
- Studies have shown the potential for PrEP to be highly effective at reducing HIV incidence among adolescent MSM, directly through use by adolescents and indirectly by reducing HIV prevalence among their sex partners Hamilton, et al. 2019; Goodreau, et al. 2018. All current PrEP options have been approved by the U.S. Food and Drug Administration (FDA) for use in adolescents aged 12 and older who weigh at least 35 kg.
- Oral PrEP:
- In May 2018, the FDA approved TDF/FTC as PrEP for adolescents weighing ≥35 kg FDA 2018. TDF/FTC as PrEP was safe and effective in adolescents, with no renal events or bone fractures noted Hosek, et al. 2017. However, there has been concern about the long-term consequences of TDF/FTC use in younger individuals who have not achieved peak bone mass. Further analysis of the ATN 110 and ATN 113 trials in adolescents during the extension phase showed that the bone loss experienced in participants aged 15 to 19 years did not recover and remained below baseline, unlike that in participants aged 20 to 22 years Havens, et al. 2020.
- TAF/FTC is FDA-approved as PrEP for cisgender male and transgender female adults and adolescents weighing ≥35kg FDA(b) 2025. Given the potential for irreversible bone loss with TDF/FTC as PrEP, it is reasonable to consider TAF/FTC as a preferred agent in adolescents aged 19 years and younger.
- CAB LA: In December 2021, CAB LA was approved by the FDA for use in adolescents ≥12 years old weighing ≥35 kg based on the inclusion of this population in the HPTN 083 and 084 trials FDA(a) 2025; Delany-Moretlwe, et al. 2022; FDA 2021; Landovitz, et al. 2021.
- SC LEN: Both the PURPOSE 1 and PURPOSE 2 trials of SC LEN as PrEP included adolescents aged 16 years and older Kelley, et al. 2025; Bekker, et al. 2024. The FDA approved SC LEN in June 2025 for use as PrEP in adolescents weighing ≥35 kg FDA(d) 2025.
All Recommendations
| ALL RECOMMENDATIONS: PREP TO PREVENT HIV AND PROMOTE SEXUAL HEALTH |
PrEP Candidates
Contraindications to PrEP
Choice of Regimen
TDF/FTC
TAF/FTC
Patients With HBV
CAB LA
SC LEN
Preinitiation Assessment
Baseline Laboratory Testing
Same-Day Initiation
Initiating PrEP During the HIV Testing Window Following Exposure
Ongoing Laboratory Testing
HIV Testing
Renal Function Testing
STI Screening
HCV Screening
Pregnancy Screening
Suspected Acute HIV
Reactive HIV Screening Test Result While Using PrEP
Ambiguous HIV Test Results
ART Selection for a Positive HIV Test Result or When Choosing to Intensify ART for an Ambiguous HIV Test Result
Discontinuing PrEP
|
Resources: Checklist 1: Key Factors in Choice of PrEP Regimen; Checklist 2: Assessment and Counseling Before PrEP Initiation; Checklist 3: Implementation Strategies for Long-Acting Injectable PrEP Regimens; Checklist 4: PrEP Initiation; Checklist 5: PrEP Follow-Up Abbreviations: Ag/Ab, antigen/antibody; APHL, Association of Public Health Laboratories; ART, antiretroviral therapy; CAB LA, long-acting injectable cabotegravir (Apretude); CDC, Centers for Disease Control and Prevention; CEI, Clinical Education Initiative; CrCl, creatinine clearance; FDA, U.S. Food and Drug Administration; HBV, hepatitis B virus; HCV, hepatitis C virus; IM, intramuscular; INSTI, integrase strand transfer inhibitor; MSM, men who have sex with men; nPEP, non-occupational post-exposure prophylaxis; oral CAB, oral cabotegravir (Vocabria); PEP, post-exposure prophylaxis; PI, protease inhibitor; PrEP, pre-exposure prophylaxis; SC LEN, subcutaneous lenacapavir (Yeztugo); STI, sexually transmitted infection; TAF/FTC, tenofovir alafenamide/emtricitabine (Descovy); TDF/FTC; tenofovir disoproxil fumarate/emtricitabine (Truvada). |
Shared Decision-Making
Download Printable PDF of Shared Decision-Making Statement
Date of current publication: August 8, 2023
Lead authors: Jessica Rodrigues, MS; Jessica M. Atrio, MD, MSc; and Johanna L. Gribble, MA
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: August 8, 2023
Rationale
Throughout its guidelines, the New York State Department of Health (NYSDOH) AIDS Institute (AI) Clinical Guidelines Program recommends “shared decision-making,” an individualized process central to patient-centered care. With shared decision-making, clinicians and patients engage in meaningful dialogue to arrive at an informed, collaborative decision about a patient’s health, care, and treatment planning. The approach to shared decision-making described here applies to recommendations included in all program guidelines. The included elements are drawn from a comprehensive review of multiple sources and similar attempts to define shared decision-making, including the Institute of Medicine’s original description [Institute of Medicine 2001]. For more information, a variety of informative resources and suggested readings are included at the end of the discussion.
Benefits
The benefits to patients that have been associated with a shared decision-making approach include:
- Decreased anxiety [Niburski, et al. 2020; Stalnikowicz and Brezis 2020]
- Increased trust in clinicians [Acree, et al. 2020; Groot, et al. 2020; Stalnikowicz and Brezis 2020]
- Improved engagement in preventive care [McNulty, et al. 2022; Scalia, et al. 2022; Bertakis and Azari 2011]
- Improved treatment adherence, clinical outcomes, and satisfaction with care [Crawford, et al. 2021; Bertakis and Azari 2011; Robinson, et al. 2008]
- Increased knowledge, confidence, empowerment, and self-efficacy [Chen, et al. 2021; Coronado-Vázquez, et al. 2020; Niburski, et al. 2020]
Approach
Collaborative care: Shared decision-making is an approach to healthcare delivery that respects a patient’s autonomy in responding to a clinician’s recommendations and facilitates dynamic, personalized, and collaborative care. Through this process, a clinician engages a patient in an open and respectful dialogue to elicit the patient’s knowledge, experience, healthcare goals, daily routine, lifestyle, support system, cultural and personal identity, and attitudes toward behavior, treatment, and risk. With this information and the clinician’s clinical expertise, the patient and clinician can collaborate to identify, evaluate, and choose from among available healthcare options [Coulter and Collins 2011]. This process emphasizes the importance of a patient’s values, preferences, needs, social context, and lived experience in evaluating the known benefits, risks, and limitations of a clinician’s recommendations for screening, prevention, treatment, and follow-up. As a result, shared decision-making also respects a patient’s autonomy, agency, and capacity in defining and managing their healthcare goals. Building a clinician-patient relationship rooted in shared decision-making can help clinicians engage in productive discussions with patients whose decisions may not align with optimal health outcomes. Fostering open and honest dialogue to understand a patient’s motivations while suspending judgment to reduce harm and explore alternatives is particularly vital when a patient chooses to engage in practices that may exacerbate or complicate health conditions [Halperin, et al. 2007].
Options: Implicit in the shared decision-making process is the recognition that the “right” healthcare decisions are those made by informed patients and clinicians working toward patient-centered and defined healthcare goals. When multiple options are available, shared decision-making encourages thoughtful discussion of the potential benefits and potential harms of all options, which may include doing nothing or waiting. This approach also acknowledges that efficacy may not be the most important factor in a patient’s preferences and choices [Sewell, et al. 2021].
Clinician awareness: The collaborative process of shared decision-making is enhanced by a clinician’s ability to demonstrate empathic interest in the patient, avoid stigmatizing language, employ cultural humility, recognize systemic barriers to equitable outcomes, and practice strategies of self-awareness and mitigation against implicit personal biases [Parish, et al. 2019].
Caveats: It is important for clinicians to recognize and be sensitive to the inherent power and influence they maintain throughout their interactions with patients. A clinician’s identity and community affiliations may influence their ability to navigate the shared decision-making process and develop a therapeutic alliance with the patient and may affect the treatment plan [KFF 2023; Greenwood, et al. 2020]. Furthermore, institutional policy and regional legislation, such as requirements for parental consent for gender-affirming care for transgender people or insurance coverage for sexual health care, may infringe upon a patient’s ability to access preventive- or treatment-related care [Sewell, et al. 2021].
Figure 1: Elements of Shared Decision-Making
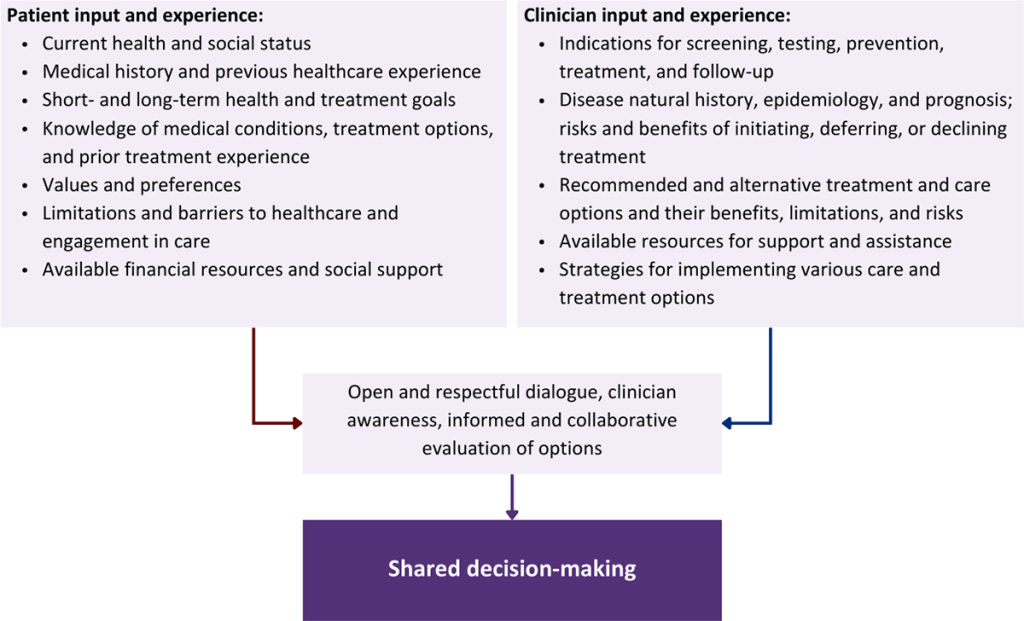
Health equity: Adapting a shared decision-making approach that supports diverse populations is necessary to achieve more equitable and inclusive health outcomes [Castaneda-Guarderas, et al. 2016]. For instance, clinicians may need to incorporate cultural- and community-specific considerations into discussions with women, gender-diverse individuals, and young people concerning their sexual behaviors, fertility intentions, and pregnancy or lactation status. Shared decision-making offers an opportunity to build trust among marginalized and disenfranchised communities by validating their symptoms, values, and lived experience. Furthermore, it can allow for improved consistency in patient screening and assessment of prevention options and treatment plans, which can reduce the influence of social constructs and implicit bias [Castaneda-Guarderas, et al. 2016].
Clinician bias has been associated with health disparities and can have profoundly negative effects [FitzGerald and Hurst 2017; Hall, et al. 2015]. It is often challenging for clinicians to recognize and set aside personal biases and to address biases with peers and colleagues. Consciously or unconsciously, negative or stigmatizing assumptions are often made about patient characteristics, such as race, ethnicity, gender, sexual orientation, mental health, and substance use [Avery, et al. 2019; van Boekel, et al. 2013; Livingston, et al. 2012]. With its emphasis on eliciting patient information, a shared decision-making approach encourages clinicians to inquire about patients’ lived experiences rather than making assumptions and to recognize the influence of that experience in healthcare decision-making.
Stigma: Stigma may prevent individuals from seeking or receiving treatment and harm reduction services [Tsai, et al. 2019]. Among people with HIV, stigma and medical mistrust remain significant barriers to healthcare utilization, HIV diagnosis, and medication adherence and can affect disease outcomes [Turan, et al. 2017; Chambers, et al. 2015], and stigma among clinicians against people who use substances has been well-documented [Stone, et al. 2021; Tsai, et al. 2019; van Boekel, et al. 2013]. Sexual and reproductive health, including strategies to prevent HIV transmission, acquisition, and progression, may be subject to stigma, bias, social influence, and violence.
| SHARED DECISION-MAKING IN HIV CARE |
|
Resources and Suggested Reading
In addition to the references cited below, the following resources and suggested reading may be useful to clinicians.
| RESOURCES |
References
Acree ME, McNulty M, Blocker O, et al. Shared decision-making around anal cancer screening among black bisexual and gay men in the USA. Cult Health Sex 2020;22(2):201-16. [PMID: 30931831]
Avery JD, Taylor KE, Kast KA, et al. Attitudes toward individuals with mental illness and substance use disorders among resident physicians. Prim Care Companion CNS Disord 2019;21(1):18m02382. [PMID: 30620451]
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med 2011;24(3):229-39. [PMID: 21551394]
Castaneda-Guarderas A, Glassberg J, Grudzen CR, et al. Shared decision making with vulnerable populations in the emergency department. Acad Emerg Med 2016;23(12):1410-16. [PMID: 27860022]
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health 2015;15:848. [PMID: 26334626]
Chen CH, Kang YN, Chiu PY, et al. Effectiveness of shared decision-making intervention in patients with lumbar degenerative diseases: a randomized controlled trial. Patient Educ Couns 2021;104(10):2498-2504. [PMID: 33741234]
Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, et al. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore) 2020;99(32):e21389. [PMID: 32769870]
Coulter A, Collins A. Making shared decision-making a reality: no decision about me, without me. 2011. https://www.kingsfund.org.uk/sites/default/files/Making-shared-decision-making-a-reality-paper-Angela-Coulter-Alf-Collins-July-2011_0.pdf
Crawford J, Petrie K, Harvey SB. Shared decision-making and the implementation of treatment recommendations for depression. Patient Educ Couns 2021;104(8):2119-21. [PMID: 33563500]
FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics 2017;18(1):19. [PMID: 28249596]
Greenwood BN, Hardeman RR, Huang L, et al. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020;117(35):21194-21200. [PMID: 32817561]
Groot G, Waldron T, Barreno L, et al. Trust and world view in shared decision making with indigenous patients: a realist synthesis. J Eval Clin Pract 2020;26(2):503-14. [PMID: 31750600]
Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health 2015;105(12):e60-76. [PMID: 26469668]
Halperin B, Melnychuk R, Downie J, et al. When is it permissible to dismiss a family who refuses vaccines? Legal, ethical and public health perspectives. Paediatr Child Health 2007;12(10):843-45. [PMID: 19043497]
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. 2001. https://www.ncbi.nlm.nih.gov/books/NBK222274/
KFF. Key data on health and health care by race and ethnicity. 2023 Mar 15. https://www.kff.org/racial-equity-and-health-policy/report/key-data-on-health-and-health-care-by-race-and-ethnicity/ [accessed 2023 May 19]
Livingston JD, Milne T, Fang ML, et al. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction 2012;107(1):39-50. [PMID: 21815959]
McNulty MC, Acree ME, Kerman J, et al. Shared decision making for HIV pre-exposure prophylaxis (PrEP) with black transgender women. Cult Health Sex 2022;24(8):1033-46. [PMID: 33983866]
Niburski K, Guadagno E, Abbasgholizadeh-Rahimi S, et al. Shared decision making in surgery: a meta-analysis of existing literature. Patient 2020;13(6):667-81. [PMID: 32880820]
Parish SJ, Hahn SR, Goldstein SW, et al. The International Society for the Study of Women’s Sexual Health process of care for the identification of sexual concerns and problems in women. Mayo Clin Proc 2019;94(5):842-56. [PMID: 30954288]
Robinson JH, Callister LC, Berry JA, et al. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008;20(12):600-607. [PMID: 19120591]
Scalia P, Durand MA, Elwyn G. Shared decision-making interventions: an overview and a meta-analysis of their impact on vaccine uptake. J Intern Med 2022;291(4):408-25. [PMID: 34700363]
Sewell WC, Solleveld P, Seidman D, et al. Patient-led decision-making for HIV preexposure prophylaxis. Curr HIV/AIDS Rep 2021;18(1):48-56. [PMID: 33417201]
Stalnikowicz R, Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract 2020;26(2):431-38. [PMID: 31989727]
Stone EM, Kennedy-Hendricks A, Barry CL, et al. The role of stigma in U.S. primary care physicians’ treatment of opioid use disorder. Drug Alcohol Depend 2021;221:108627. [PMID: 33621805]
Tsai AC, Kiang MV, Barnett ML, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med 2019;16(11):e1002969. [PMID: 31770387]
Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav 2017;21(1):283-91. [PMID: 27272742]
van Boekel LC, Brouwers EP, van Weeghel J, et al. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013;131(1-2):23-35. [PMID: 23490450]
References
Anderson P. L., Glidden D. V., Liu A., et al. Emtricitabine-tenofovir concentrations and pre-exposure prophylaxis efficacy in men who have sex with men. Sci Transl Med 2012;4(151):151ra125. [PMID: 22972843]
Apoola A., Ahmad S., Radcliffe K. Primary HIV infection. Int J STD AIDS 2002;13(2):71-78. [PMID: 11839160]
Badell M. L., Prabhu M., Dionne J., et al. Society for Maternal-Fetal Medicine Consult Series #69: Hepatitis B in pregnancy: updated guidelines. Am J Obstet Gynecol 2024;230(4):B2-11. [PMID: 38141870]
Baeten J. M., Donnell D., Ndase P., et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med 2012;367(5):399-410. [PMID: 22784037]
Bavinton B. R., Pinto A. N., Phanuphak N., et al. Viral suppression and HIV transmission in serodiscordant male couples: an international, prospective, observational, cohort study. Lancet HIV 2018;5(8):e438-47. [PMID: 30025681]
Bazzi A. R., Biancarelli D. L., Childs E., et al. Limited knowledge and mixed interest in pre-exposure prophylaxis for HIV prevention among people who inject drugs. AIDS Patient Care STDS 2018;32(12):529-37. [PMID: 30311777]
Bekker L. G., Das M., Abdool Karim Q., et al. Twice-yearly lenacapavir or daily F/TAF for HIV prevention in cisgender women. N Engl J Med 2024;391(13):1179-92. [PMID: 39046157]
Blair C. S., Li S., Chau G., et al. Brief report: hormonal contraception use and cabotegravir pharmacokinetics in HIV-uninfected women enrolled in HPTN 077. J Acquir Immune Defic Syndr 2020;85(1):93-97. [PMID: 32452972]
Blumenthal J., Goyal R., Burke L., et al. The bidirectional effects of hormone therapy and PrEP in transgender individuals. CROI; 2022 Feb 12-16; Virtual. https://www.croiconference.org/abstract/the-bidirectional-effects-of-hormone-therapy-and-prep-in-transgender-individuals/
Bradshaw D., Matthews G., Danta M. Sexually transmitted hepatitis C infection: the new epidemic in MSM?. Curr Opin Infect Dis 2013;26(1):66-72. [PMID: 23242342]
Buchacz K., McFarland W., Kellogg T. A., et al. Amphetamine use is associated with increased HIV incidence among men who have sex with men in San Francisco. AIDS 2005;19(13):1423-24. [PMID: 16103774]
Bujan L., Pasquier C. People living with HIV and procreation: 30 years of progress from prohibition to freedom?. Hum Reprod 2016;31(5):918-25. [PMID: 26975324]
Buti M., Casillas R., Riveiro-Barciela M., et al. Tenofovir discontinuation after long-term viral suppression in HBeAg negative chronic hepatitis B. Can HBsAg levels be useful?. J Clin Virol 2015;68:61-68. [PMID: 26071338]
Calabrese S. K., Earnshaw V. A., Underhill K., et al. The impact of patient race on clinical decisions related to prescribing HIV pre-exposure prophylaxis (PrEP): assumptions about sexual risk compensation and implications for access. AIDS Behav 2014;18(2):226-40. [PMID: 24366572]
Calabrese S. K., Earnshaw V. A., Underhill K., et al. Prevention paradox: medical students are less inclined to prescribe HIV pre-exposure prophylaxis for patients in highest need. J Int AIDS Soc 2018;21(6):e25147. [PMID: 29939488]
Celum C., Morrow R. A., Donnell D., et al. Daily oral tenofovir and emtricitabine-tenofovir preexposure prophylaxis reduces herpes simplex virus type 2 acquisition among heterosexual HIV-1-uninfected men and women: a subgroup analysis of a randomized trial. Ann Intern Med 2014;161(1):11-19. [PMID: 24979446]
Chamorro A. J., Casado J. L., Bellido D., et al. Reactivation of hepatitis B in an HIV-infected patient with antibodies against hepatitis B core antigen as the only serological marker. Eur J Clin Microbiol Infect Dis 2005;24(7):492-94. [PMID: 15990987]
Chawki S., Goldwirt L., Mouhebb M. E., et al. Ex-vivo rectal tissue infection with HIV-1 to assess time to protection following oral preexposure prophylaxis with tenofovir disoproxil/emtricitabine. AIDS 2024;38(4):455-64. [PMID: 37976073]
Chin T., Hicks C., Samsa G., et al. Diagnosing HIV infection in primary care settings: missed opportunities. AIDS Patient Care STDS 2013;27(7):392-97. [PMID: 23802143]
Choopanya K., Martin M., Suntharasamai P., et al. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2013;381(9883):2083-90. [PMID: 23769234]
CMS. Fact sheet: Medicare part B coverage of pre-exposure prophylaxis (PrEP) for human immunodeficiency virus (HIV) prevention. 2024 Sep 30. https://www.cms.gov/files/document/fact-sheet-potential-medicare-part-b-coverage-preexposure-prophylaxis-prep-using-antiretroviral.pdf [accessed 2025 Aug 18]
Cockbain B., Whitlock G., Dean Street Collaborative Group. Immediate PrEP when accessing PEP: a service evaluation. HIV Med 2022;23(10):1108-12. [PMID: 35352455]
Cohen M. S., Chen Y. Q., McCauley M., et al. Antiretroviral therapy for the prevention of HIV-1 transmission. N Engl J Med 2016;375(9):830-39. [PMID: 27424812]
Cottrell M. L., Prince H. M. A., Schauer A. P., et al. Decreased tenofovir diphosphate concentrations in a transgender female cohort: implications for HIV pre-exposure prophylaxis (PrEP). Clin Infect Dis 2019;69(12):2201-4. [PMID: 30963179]
Cottrell M. L., Yang K. H., Prince H. M., et al. A translational pharmacology approach to predicting outcomes of preexposure prophylaxis against HIV in men and women using tenofovir disoproxil fumarate with or without emtricitabine. J Infect Dis 2016;214(1):55-64. [PMID: 26917574]
Cox S., Parikh U. M., Heaps A. L., et al. Deep sequencing with unique molecular identifiers for evaluation of HIV-1 drug resistance in the DISCOVER pre-exposure prophylaxis trial. Abstract PDB0404. J Int AIDS Soc 2020;23(S4):118. https://pubmed.ncbi.nlm.nih.gov/32649039
Dawit R., Goedel W. C., Reid S. C., et al. Geographic variations of pre-exposure prophylaxis reversal and abandonment among United States counties. AIDS 2024;38(4):557-66. [PMID: 37976040]
Delaney K. P., Hanson D. L., Masciotra S., et al. Time until emergence of HIV test reactivity following infection with HIV-1: implications for interpreting test results and retesting after exposure. Clin Infect Dis 2017;64(1):53-59. [PMID: 27737954]
Delany-Moretlwe S., Hanscom B., Guo X., et al. Evaluation of long-acting cabotegravir safety and pharmacokinetics in pregnant women in eastern and southern Africa: a secondary analysis of HPTN 084. J Int AIDS Soc 2025;28(1):e26401. [PMID: 39748218]
Delany-Moretlwe S., Hughes J. P., Bock P., et al. Cabotegravir for the prevention of HIV-1 in women: results from HPTN 084, a phase 3, randomised clinical trial. Lancet 2022;399(10337):1779-89. [PMID: 35378077]
Deutsch M. B., Glidden D. V., Sevelius J., et al. HIV pre-exposure prophylaxis in transgender women: a subgroup analysis of the iPrEx trial. Lancet HIV 2015;2(12):e512-19. [PMID: 26614965]
Dize L., Barnes P., Barnes M., et al. Performance of self-collected penile-meatal swabs compared to clinician-collected urethral swabs for the detection of Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and Mycoplasma genitalium by nucleic acid amplification assays. Diagn Microbiol Infect Dis 2016;86(2):131-35. [PMID: 27497595]
Dore G. J., Soriano V., Rockstroh J., et al. Frequent hepatitis B virus rebound among HIV-HBV-coinfected patients following antiretroviral therapy interruption in the SMART study. AIDS 2010;24(6):857-65. [PMID: 20216301]
Drake A. L., Wagner A., Richardson B., et al. Incident HIV during pregnancy and postpartum and risk of mother-to-child HIV transmission: a systematic review and meta-analysis. PLoS Med 2014;11(2):e1001608. [PMID: 24586123]
Edelman E. J., Moore B. A., Calabrese S. K., et al. Primary care physicians' willingness to prescribe HIV pre-exposure prophylaxis for people who inject drugs. AIDS Behav 2017;21(4):1025-33. [PMID: 27896552]
Ehrhardt S., Xie C., Guo N., et al. Breastfeeding while taking lamivudine or tenofovir disoproxil fumarate: a review of the evidence. Clin Infect Dis 2015;60(2):275-78. [PMID: 25313254]
Ending the Epidemic Dashboard. Using metrics to track New York State’s progress towards ending the HIV epidemic. 2025 Sep 29. https://etedashboardny.org/ [accessed 2025 Aug 15]
Engel N., Dumond J. B., Kashuba A. D. M., et al. Optimizing on-demand tenofovir disoproxil fumarate/emtricitabine dosing in women for HIV prevention. J Infect Dis 2025. https://doi.org/10.1093/infdis/jiaf459
Eshleman S. H., Fogel J. M., Piwowar-Manning E., et al. Characterization of human immunodeficiency virus (HIV) infections in women who received injectable cabotegravir or tenofovir disoproxil fumarate/emtricitabine for HIV prevention: HPTN 084. J Infect Dis 2022;225(10):1741-49. [PMID: 35301540]
FDA. Supplement approval for Truvada. 2018 May 15. https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2018/021752Orig1s055ltr.pdf [accessed 2025 Aug 19]
FDA. FDA clears first diagnostic tests for extragenital testing for chlamydia and gonorrhea. 2019 May 23. https://www.fda.gov/news-events/press-announcements/fda-clears-first-diagnostic-tests-extragenital-testing-chlamydia-and-gonorrhea [accessed 2025 Aug 19]
FDA. FDA approves first injectable treatment for HIV pre-exposure prevention. 2021 Dec 20. https://www.fda.gov/news-events/press-announcements/fda-approves-first-injectable-treatment-hiv-pre-exposure-prevention [accessed 2025 Aug 15]
FDA. Truvada (emtricitabine and tenofovir disoproxil fumarate) tablets, for oral use. 2024 Apr. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/021752s064lbl.pdf [accessed 2025 Aug 18]
FDA(a). Apretude (cabotegravir extended-release injectable suspension), for intramuscular use. 2025 Apr. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215499s009lbl.pdf [accessed 2025 Aug 19]
FDA(b). Descovy (emtricitabine and tenofovir alafenamide) tablets, for oral use. 2025 Jun. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/208215s023s025lbl.pdf [accessed 2025 Aug 15]
FDA(c). Vocabria (cabotegravir) tablets, for oral use. 2025 Apr. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/212887s011lbl.pdf [accessed 2025 Aug 19]
FDA(d). Yeztugo (lenacapavir) tablets, for oral use; injection, for subcutaneous use. 2025 Jun. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/220020s000lbl.pdf [accessed 2025 Aug 19]
Fierer D. S., Factor S. H. Defining the scope of sexually transmitted hepatitis C virus epidemic among HIV-infected men who have sex with men in New York City. Sex Transm Dis 2015;42(7):400-401. [PMID: 26222756]
Gandhi M., Glidden D. V., Mayer K., et al. Association of age, baseline kidney function, and medication exposure with declines in creatinine clearance on pre-exposure prophylaxis: an observational cohort study. Lancet HIV 2016;3(11):e521-28. [PMID: 27658870]
Gibas K. M., van den Berg P., Powell V. E., et al. Drug resistance during HIV pre-exposure prophylaxis. Drugs 2019;79(6):609-19. [PMID: 30963509]
Gilead. Yeztugo (lenacapavir) oral initiation dosing requirement. 2025. https://www.askgileadmedical.com/docs/yeztugo/yeztugo-oral-initiation-dosing-requirement [accessed 2025 Aug 19]
Girometti N., McCormack S., Tittle V., et al. Rising rates of recent PrEP exposure among MSM newly diagnosed with HIV: antiviral resistance patterns and treatment outcomes. AIDS 2022;36(4):561-66. [PMID: 34873084]
Glidden D. V., Amico K. R., Liu A. Y., et al. Symptoms, side effects and adherence in the iPrEx open-label extension. Clin Infect Dis 2016;62(9):1172-77. [PMID: 26797207]
Golub S. A., Pena S., Boonrai K., et al. STI data from community-based PrEP implementation suggest changes to CDC guidelines. CROI; 2016 Feb 22-25; Boston, MA. http://www.croiconference.org/sessions/sti-data-community-based-prep-implementation-suggest-changes-cdc-guidelines-0
Goodreau S. M., Hamilton D. T., Jenness S. M., et al. Targeting human immunodeficiency virus pre-exposure prophylaxis to adolescent sexual minority males in higher prevalence areas of the United States: a modeling study. J Adolesc Health 2018;62(3):311-19. [PMID: 29248392]
Grant R. M., Anderson P. L., McMahan V., et al. Uptake of pre-exposure prophylaxis, sexual practices, and HIV incidence in men and transgender women who have sex with men: a cohort study. Lancet Infect Dis 2014;14(9):820-29. [PMID: 25065857]
Grant R. M., Lama J. R., Anderson P. L., et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med 2010;363(27):2587-99. [PMID: 21091279]
Grant R. M., Pellegrini M., Defechereux P. A., et al. Sex hormone therapy and tenofovir diphosphate concentration in dried blood spots: primary results of the interactions between antiretrovirals and transgender hormones study. Clin Infect Dis 2021;73(7):e2117-23. [PMID: 32766890]
Grinsztejn B., Hoagland B., Coutinho C., et al. ImPrEP CAB Brasil: enhancing PrEP coverage with CAB-LA in young key populations. Abstract 192. CROI; 2025 Mar 9-12; San Francisco, CA. https://www.croiconference.org/abstract/3614-2025/
Grov C., Rendina H. J., Ventuneac A., et al. HIV risk in group sexual encounters: an event-level analysis from a national online survey of MSM in the U.S. J Sex Med 2013;10(9):2285-94. [PMID: 23809410]
Guo Y., Westmoreland D. A., D'Angelo A., et al. PrEP discontinuation in a US national cohort of sexual and gender minority populations, 2017-22. Health Aff (Millwood) 2024;43(3):443-51. [PMID: 38437609]
Hamilton D. T., Rosenberg E. S., Jenness S. M., et al. Modeling the joint effects of adolescent and adult PrEP for sexual minority males in the United States. PLoS One 2019;14(5):e0217315. [PMID: 31116802]
Han(a) K., Patel P., McCallister S., et al. Long-acting cabotegravir pharmacokinetics with and without oral lead-in for HIV PrEP. Antimicrob Agents Chemother 2024;68(6):e0147523. [PMID: 38709006]
Han(b) K., D'Amico R., Spreen W., et al. Model-based comparison of cabotegravir pharmacokinetics following thigh and gluteal injections. Abstract 617. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/model-based-comparison-of-cabotegravir-pharmacokinetics-following-thigh-and-gluteal-injections/
Harris M. T., Weinberger E., O'Brien C., et al. PrEP facilitators and barriers in substance use bridge clinics for women who engage in sex work and who use drugs. Addict Sci Clin Pract 2024;19(1):47. [PMID: 38831359]
Havens P. L., Perumean-Chaney S. E., Patki A., et al. Changes in bone mass after discontinuation of pre-exposure prophylaxis (PrEP) with tenofovir disoproxil fumarate/emtricitabine in young men who have sex with men: extension phase results of Adolescent Trials Network Protocols 110 and 113. Clin Infect Dis 2020;70(4):687-91. [PMID: 31179503]
Heffron R., Mugo N., Hong T., et al. Pregnancy outcomes and infant growth among babies with in-utero exposure to tenofovir-based preexposure prophylaxis for HIV prevention. AIDS 2018;32(12):1707-13. [PMID: 30001244]
Heffron R., Pintye J., Matthews L. T., et al. PrEP as peri-conception HIV prevention for women and men. Curr HIV/AIDS Rep 2016;13(3):131-39. [PMID: 26993627]
Hendrix C. W., Andrade A., Bumpus N. N., et al. Dose frequency ranging pharmacokinetic study of tenofovir-emtricitabine after directly observed dosing in healthy volunteers to establish adherence benchmarks (HPTN 066). AIDS Res Hum Retroviruses 2016;32(1):32-43. [PMID: 26414912]
Heuker J., Sonder G. J., Stolte I., et al. High HIV incidence among MSM prescribed postexposure prophylaxis, 2000-2009: indications for ongoing sexual risk behaviour. Aids 2012;26(4):505-12. [PMID: 22156963]
Hill A., Hughes S. L., Gotham D., et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate: is there a true difference in efficacy and safety?. J Virus Erad 2018;4(2):72-79. [PMID: 29682298]
Hiransuthikul A., Janamnuaysook R., Himmad K., et al. Drug-drug interactions between feminizing hormone therapy and pre-exposure prophylaxis among transgender women: the iFACT study. J Int AIDS Soc 2019;22(7):e25338. [PMID: 31298497]
Hiransuthikul A., Thammajaruk N., Kerr S., et al. No significant drug-drug interaction between oral TAF-based PrEP and feminizing hormone therapy among transgender women in Thailand: the iFACT-3 study. J Int AIDS Soc 2025;28(5):e26502. [PMID: 40390323]
Hoornenborg(a) E., Prins M., Achterbergh R. C. A., et al. Acquisition of wild-type HIV-1 infection in a patient on pre-exposure prophylaxis with high intracellular concentrations of tenofovir diphosphate: a case report. Lancet HIV 2017;4(11):e522-28. [PMID: 28919303]
Hoornenborg(b) E., Achterbergh R. C. A., Schim Van Der Loeff M. F., et al. MSM starting preexposure prophylaxis are at risk of hepatitis C virus infection. AIDS 2017;31(11):1603-10. [PMID: 28657964]
Hosek S. G., Rudy B., Landovitz R., et al. An HIV preexposure prophylaxis demonstration project and safety study for young MSM. J Acquir Immune Defic Syndr 2017;74(1):21-29. [PMID: 27632233]
Jenness S. M., Goodreau S. M., Rosenberg E., et al. Impact of the Centers for Disease Control's HIV preexposure prophylaxis guidelines for men who have sex with men in the United States. J Infect Dis 2016;214(12):1800-1807. [PMID: 27418048]
Jenness S. M., Weiss K. M., Goodreau S. M., et al. Incidence of gonorrhea and chlamydia following human immunodeficiency virus preexposure prophylaxis among men who have sex with men: a modeling study. Clin Infect Dis 2017;65(5):712-18. [PMID: 28505240]
Jogiraju V., Pawar P., Yager J., et al. Pharmacokinetics and safety of once-yearly lenacapavir: a phase 1, open-label study. Lancet 2025;405(10485):1147-54. [PMID: 40086460]
Joseph Davey D., Dadan S., Wara N. Transforming HIV prevention: the promise of long-acting preexposure prophylaxis in high HIV burden settings. Curr Opin HIV AIDS 2025;20(1):32-38. [PMID: 39561011]
Kamis K. F., Marx G. E., Scott K. A., et al. Same-day HIV pre-exposure prophylaxis (PrEP) initiation during drop-in sexually transmitted diseases clinic appointments is a highly acceptable, feasible, and safe model that engages individuals at risk for HIV into PrEP care. Open Forum Infect Dis 2019;6(7):ofz310. [PMID: 31341933]
Kamya M. R., Balzer L. B., Ayieko J., et al. Dynamic choice HIV prevention with cabotegravir long-acting injectable in rural Uganda and Kenya: a randomised trial extension. Lancet HIV 2024;11(11):e736-45. [PMID: 39395424]
Kelley C. F., Acevedo-Quinones M., Agwu A. L., et al. Twice-yearly lenacapavir for HIV prevention in men and gender-diverse persons. N Engl J Med 2025;392(13):1261-76. [PMID: 39602624]
Kiweewa F. M., Ahmed K., Nair G., et al. Adherence to F/TAF in cisgender women prevents HIV with low risk of resistance or diagnostic delay. Abstract 194. CROI; 2025 Mar 9-12; San Francisco, CA. https://www.croiconference.org/abstract/1937-2025/
Knox D. C., Anderson P. L., Harrigan P. R., et al. Multidrug-resistant HIV-1 infection despite preexposure prophylaxis. N Engl J Med 2017;376(5):501-2. [PMID: 28146652]
Koblin B. A., Mansergh G., Frye V., et al. Condom-use decision making in the context of hypothetical pre-exposure prophylaxis efficacy among substance-using men who have sex with men: Project MIX. J Acquir Immune Defic Syndr 2011;58(3):319-27. [PMID: 21765363]
Koren D. E., Fedkiv V., Zhao H., et al. Perceptions of long-acting injectable antiretroviral treatment regimens in a United States urban academic medical center. J Int Assoc Provid AIDS Care 2020;19:2325958220981265. [PMID: 33327851]
LaLota M., Beck D. W., Metsch L. R., et al. HIV seropositivity and correlates of infection among heterosexually active adults in high-risk areas in South Florida. AIDS Behav 2011;15(6):1259-63. [PMID: 21153433]
Lampe M. A., Smith D. K., Anderson G. J., et al. Achieving safe conception in HIV-discordant couples: the potential role of oral preexposure prophylaxis (PrEP) in the United States. Am J Obstet Gynecol 2011;204(6):488.e1-8. [PMID: 21457911]
Landovitz R. J., Donnell D., Clement M. E., et al. Cabotegravir for HIV prevention in cisgender men and transgender women. N Engl J Med 2021;385(7):595-608. [PMID: 34379922]
Landovitz R. J., Donnell D., Tran H., et al. Updated efficacy, safety, and case studies in HPTN 083: CAB-LA vs TDF/FTC for PrEP. CROI; 2022 Feb 12-16; Virtual. https://www.croiconference.org/abstract/updated-efficacy-safety-and-case-studies-in-hptn-083-cab-la-vs-tdf-ftc-for-prep/
Landovitz R. J., Li S., Eron J. J., et al. Tail-phase safety, tolerability, and pharmacokinetics of long-acting injectable cabotegravir in HIV-uninfected adults: a secondary analysis of the HPTN 077 trial. Lancet HIV 2020;7(7):e472-81. [PMID: 32497491]
Landovitz(a) R. J., Delany-Moretlwe S., Fogel J. M., et al. Features of HIV infection in the context of long-acting cabotegravir preexposure prophylaxis. N Engl J Med 2024;391(13):1253-56. [PMID: 39046350]
Landovitz(b) R., Gao F., Fogel J. M., et al. Performance characteristics of HIV RNA screening with long-acting injectable cabotegravir (CAB-LA) pre-exposure prophylaxis (PrEP) in the multicenter global HIV Prevention Trials Network 083 (HPTN 083) Study. Abstract OAE0406LB. 25th International AIDS Conference; 2024 Jul 20-26; Munich, Germany. https://www.natap.org/2024/IAS/IAS_02.htm
Lat A. K., Kim A., Zhang H., et al. 1542. Impact of subcutaneous administration sites on the clinical pharmacokinetics of lenacapavir, a long-acting HIV capsid inhibitor: does body site matter?. Open Forum Infect Dis 2023;10:ofad500.1377. https://pmc.ncbi.nlm.nih.gov/articles/PMC10678519/
Lehman D. A., Baeten J. M., McCoy C. O., et al. Risk of drug resistance among persons acquiring HIV within a randomized clinical trial of single- or dual-agent preexposure prophylaxis. J Infect Dis 2015;211(8):1211-18. [PMID: 25587020]
Liegeon G., Brun A., Hamet G., et al. Brief report: incidence and management of complex kidney situations among on-demand and daily HIV pre-exposure prophylaxis users. J Acquir Immune Defic Syndr 2024;95(3):255-59. [PMID: 37977193]
Liotta G., Floridia M., Andreotti M., et al. Growth indices in breastfed infants pre and postnatally exposed to tenofovir compared with tenofovir-unexposed infants. Aids 2016;30(3):525-27. [PMID: 26765942]
Liu A. Y., Cohen S. E., Vittinghoff E., et al. Preexposure prophylaxis for HIV infection integrated with municipal- and community-based sexual health services. JAMA Intern Med 2016;176(1):75-84. [PMID: 26571482]
Louissaint N. A., Cao Y. J., Skipper P. L., et al. Single dose pharmacokinetics of oral tenofovir in plasma, peripheral blood mononuclear cells, colonic tissue, and vaginal tissue. AIDS Res Hum Retroviruses 2013;29(11):1443-50. [PMID: 23600365]
Lunny C., Taylor D., Hoang L., et al. Self-collected versus clinician-collected sampling for chlamydia and gonorrhea screening: a systemic review and meta-analysis. PLoS One 2015;10(7):e0132776. [PMID: 26168051]
Malone J., Reisner S. L., Cooney E. E., et al. Perceived HIV acquisition risk and low uptake of PrEP among a cohort of transgender women with prep indication in the Eastern and Southern United States. J Acquir Immune Defic Syndr 2021;88(1):10-18. [PMID: 34397742]
Markowitz M., Grossman H., Anderson P. L., et al. Newly acquired infection with multidrug-resistant HIV-1 in a patient adherent to preexposure prophylaxis. J Acquir Immune Defic Syndr 2017;76(4):e104-6. [PMID: 29076941]
Martin E. G., MacDonald R. H., Gordon D. E., et al. Simulating the end of AIDS in New York: using participatory dynamic modeling to improve implementation of the ending the epidemic initiative. Public Health Rep 2020;135(1_suppl):158S-71S. [PMID: 32735199]
Marzinke M. A., Fogel J. M., Wang Z., et al. Extended analysis of HIV infection in cisgender men and transgender women who have sex with men receiving injectable cabotegravir for HIV prevention: HPTN 083. Antimicrob Agents Chemother 2023;67(4):e0005323. [PMID: 36995219]
Marzinke(a) M., Grinsztejn B., Fogel J. M., et al. Characterization of human immunodeficiency virus (HIV) infection in cisgender men and transgender women who have sex with men receiving injectable cabotegravir for HIV prevention: HPTN 083. J Infect Dis 2021;224(9):1581-92. [PMID: 33740057]
Marzinke(b) M., Delany-Moretlwe S., Agyei Y., et al. Long-acting injectable PrEP in women: laboratory analysis of HIV infections in HPTN 084. IAS; 2021 Jul 18-21; Virtual. https://theprogramme.ias2021.org/Abstract/Abstract/2606
Mayer K. H., Grasso C., Levine K., et al. Increasing PrEP uptake, persistent disparities in at-risk patients in a Boston center. CROI; 2018 Mar 4-7; Boston, MA. http://www.croiconference.org/sessions/increasing-prep-uptake-persistent-disparities-risk-patients-boston-center
Mayer K. H., Molina J. M., Thompson M. A., et al. Emtricitabine and tenofovir alafenamide vs emtricitabine and tenofovir disoproxil fumarate for HIV pre-exposure prophylaxis (DISCOVER): primary results from a randomised, double-blind, multicentre, active-controlled, phase 3, non-inferiority trial. Lancet 2020;396(10246):239-54. [PMID: 32711800]
McCormack S., Dunn D. T., Desai M., et al. Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (PROUD): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet 2016;387(10013):53-60. [PMID: 26364263]
Mikati T., Jamison K., Daskalakis D. C. Immediate PrEP initiation at New York City sexual health clinics. CROI; 2019 Mar 4-7. http://www.croiconference.org/sessions/immediate-prep-initiation-new-york-city-sexual-health-clinics
Mistler C. B., Copenhaver M. M., Shrestha R. The pre-exposure prophylaxis (PrEP) care cascade in people who inject drugs: a systematic review. AIDS Behav 2021;25(5):1490-1506. [PMID: 32749627]
Molina J. M., Capitant C., Spire B., et al. On-demand preexposure prophylaxis in men at high risk for HIV-1 infection. N Engl J Med 2015;373(23):2237-46. [PMID: 26624850]
Molina J. M., Ghosn J., Assoumou L., et al. Daily and on-demand HIV pre-exposure prophylaxis with emtricitabine and tenofovir disoproxil (ANRS PREVENIR): a prospective observational cohort study. Lancet HIV 2022;9(8):e554-62. [PMID: 35772417]
Mujugira A., Celum C., Coombs R. W., et al. HIV transmission risk persists during the first 6 months of antiretroviral therapy. J Acquir Immune Defic Syndr 2016;72(5):579-84. [PMID: 27070123]
Murray M. I., Markowitz M., Frank I., et al. Satisfaction and acceptability of cabotegravir long-acting injectable suspension for prevention of HIV: patient perspectives from the ECLAIR trial. HIV Clin Trials 2018;19(4):129-138. [PMID: 30445896]
NYSDOH. Unpublished data; 2023.
Ogbuagu O., Ruane P. J., Podzamczer D., et al. Long-term safety and efficacy of emtricitabine and tenofovir alafenamide vs emtricitabine and tenofovir disoproxil fumarate for HIV-1 pre-exposure prophylaxis: week 96 results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet HIV 2021;8(7):e397-407. [PMID: 34197772]
Orkin C., Bernal Morell E., Tan D. H. S., et al. Initiation of long-acting cabotegravir plus rilpivirine as direct-to-injection or with an oral lead-in in adults with HIV-1 infection: week 124 results of the open-label phase 3 FLAIR study. Lancet HIV 2021;8(11):e668-78. [PMID: 34656207]
Patel N., Morris S., Burke L., et al. No observed bidirectional effect between tenofovir diphosphate concentrations and gender-affirming hormone concentrations among transgender persons switching from tenofovir disoproxil fumarate/emtricitabine to tenofovir alafenamide/emtricitabine for HIV pre-exposure prophylaxis. Br J Clin Pharmacol 2024;90(10):2360-65. [PMID: 38646796]
Patterson K. B., Prince H. A., Kraft E., et al. Penetration of tenofovir and emtricitabine in mucosal tissues: implications for prevention of HIV-1 transmission. Sci Transl Med 2011;3(112):112re4. [PMID: 22158861]
Patton M. E., Kidd S., Llata E., et al. Extragenital gonorrhea and chlamydia testing and infection among men who have sex with men--STD Surveillance Network, United States, 2010–2012. Clin Infect Dis 2014;58(11):1564-70. [PMID: 24647015]
Philbin M. M., Parish C., Bergen S., et al. A qualitative exploration of women's interest in long-acting injectable antiretroviral therapy across six cities in the women's interagency HIV study: intersections with current and past injectable medication and substance use. AIDS Patient Care STDS 2021;35(1):23-30. [PMID: 33400587]
Phillips A. N., Hickey M., Shade S., et al. Dynamic choice HIV prevention with cabotegravir (CAB-LA): a model-based cost-effectiveness analysis. CROI; 2025 Mar 9-12; San Francisco, CA. https://www.croiconference.org/abstract/848-2025/
Pilkington V., Hill A., Hughes S., et al. How safe is TDF/FTC as PrEP? A systematic review and meta-analysis of the risk of adverse events in 13 randomised trials of PrEP. J Virus Erad 2018;4(4):215-24. [PMID: 30515300]
Pitasi M. A., Kerani R. P., Kohn R., et al. Chlamydia, gonorrhea, and human immunodeficiency virus infection among transgender women and transgender men attending clinics that provide sexually transmitted disease services in six US cities: results from the Sexually Transmitted Disease Surveillance Network. Sex Transm Dis 2019;46(2):112-17. [PMID: 30278030]
Price J. C., McKinney J. E., Crouch P. C., et al. Sexually acquired hepatitis C infection in HIV-uninfected men who have sex with men using pre-exposure prophylaxis against HIV. J Infect Dis 2019;219(9):1373-76. [PMID: 30462305]
Rael C. T., Martinez M., Giguere R., et al. Transgender women's concerns and preferences on potential future long-acting biomedical HIV prevention strategies: the case of injections and implanted medication delivery devices (IMDDs). AIDS Behav 2020;24(5):1452-62. [PMID: 31654172]
Reddy K., Naidoo K. L., Lombard C., et al. In-utero exposure to tenofovir-containing pre-exposure prophylaxis and bone mineral content in HIV-unexposed infants in South Africa. J Int AIDS Soc 2024;27(11):e26379. [PMID: 39528419]
Reed J. B., Shrestha P., Were D., et al. HIV PrEP is more than ART-lite: longitudinal study of real-world PrEP services data identifies missing measures meaningful to HIV prevention programming. J Int AIDS Soc 2021;24(10):e25827. [PMID: 34648678]
Reisner S. L., Pletta D. R., Mayer K. H., et al. HIV seropositivity and viral non-suppression in transgender, non-binary, and gender-diverse people in primary care receiving gender-affirming hormone therapy in the USA between 2013 and 2019 (LEGACY): an observational, longitudinal, cohort study. Lancet HIV 2025;12(4):e283-92. [PMID: 40158515]
Ribas Rietti Souto A., Aikhuele E., Esposito M., et al. Patient and provider perceptions of barriers and facilitators to pre-exposure prophylaxis access and adherence in Black and Latinx young men who have sex with men. AIDS Patient Care STDS 2024;38(7):315-23. [PMID: 38916119]
Rizzardini G., Overton E. T., Orkin C., et al. Long-acting injectable cabotegravir + rilpivirine for HIV maintenance therapy: week 48 pooled analysis of phase 3 ATLAS and FLAIR trials. J Acquir Immune Defic Syndr 2020;85(4):498-506. [PMID: 33136751]
Rodger A. J., Cambiano V., Bruun T., et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet 2019;393(10189):2428-38. [PMID: 31056293]
Rodger A. J., Cambiano V., Bruun T., et al. Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy. JAMA 2016;316(2):171-81. [PMID: 27404185]
Russ S., Zhang C., Liu Y. Pre-exposure prophylaxis care continuum, barriers, and facilitators among black men who have sex with men in the United States: a systematic review and meta-analysis. AIDS Behav 2021;25(7):2278-88. [PMID: 33438151]
Salvadori N., Fan B., Teeyasoontranon W., et al. Maternal and infant bone mineral density 1 year after delivery in a randomized, controlled trial of maternal tenofovir disoproxil fumarate to prevent mother-to-child transmission of hepatitis B virus. Clin Infect Dis 2019;69(1):144-46. [PMID: 30924492]
Saunders G., Mortensen E., Shen G., et al. Injection site reactions with subcutaneous lenacapavir administration at alternate injection sites. 25th International AIDS Conference; 2024 Jul 22-26; Munich, Germany. https://www.hivandmore.de/kongresse/weltaids2024/pdf/gilead/Saunders_AIDS2024_Poster_THPEB103.pdf
Scheim A. I., Bauer G. R., Travers R. HIV-related sexual risk among transgender men who are gay, bisexual, or have sex with men. J Acquir Immune Defic Syndr 2017;74(4):e89-96. [PMID: 27798432]
Scott H. M., Spinelli M., Vittinghoff E., et al. Racial/ethnic and HIV risk category disparities in preexposure prophylaxis discontinuation among patients in publicly funded primary care clinics. AIDS 2019;33(14):2189-95. [PMID: 31436610]
Seifert S. M., Chen X., Meditz A. L., et al. Intracellular tenofovir and emtricitabine anabolites in genital, rectal, and blood compartments from first dose to steady state. AIDS Res Hum Retroviruses 2016;32(10-11):981-91. [PMID: 27526873]
Senneker T. Drug-drug interactions between gender-affirming hormone therapy and antiretrovirals for treatment/prevention of HIV. Br J Clin Pharmacol 2024;90(10):2366-82. [PMID: 38866600]
Sevelius J. M., Deutsch M. B., Grant R. The future of PrEP among transgender women: the critical role of gender affirmation in research and clinical practices. J Int AIDS Soc 2016;19(7 Suppl 6):21105. [PMID: 27760683]
Sharpe J. D., Siegler A. J., Sanchez T. H., et al. Effects of mode of transportation on PrEP persistence among urban men who have sex with men. AIDS Care 2023;35(9):1411-19. [PMID: 37232114]
Shieh E., Marzinke M. A., Fuchs E. J., et al. Transgender women on oral HIV pre-exposure prophylaxis have significantly lower tenofovir and emtricitabine concentrations when also taking oestrogen when compared to cisgender men. J Int AIDS Soc 2019;22(11):e25405. [PMID: 31692269]
Siberry G. K., Jacobson D. L., Kalkwarf H. J., et al. Lower newborn bone mineral content associated with maternal use of tenofovir disoproxil fumarate during pregnancy. Clin Infect Dis 2015;61(6):996-1003. [PMID: 26060285]
Siegler A. J., Mayer K. H., Liu A. Y., et al. Developing and assessing the feasibility of a home-based PrEP monitoring and support program. Clin Infect Dis 2019;63(3):501-4. [PMID: 29982304]
Singh S., Lampe M. A., Surendera A. B., et al. HIV seroconversion during pregnancy and mother-to-child HIV transmission: data from the Enhanced Perinatal Surveillance Project, United States, 2005-2010. THAC0104. JIAS 2012;15:130-31. https://studylib.net/doc/18607036/--journal-of-the-international-aids-society
Smith D. K., Pals S. L., Herbst J. H., et al. Development of a clinical screening index predictive of incident HIV infection among men who have sex with men in the United States. J Acquir Immune Defic Syndr 2012;60(4):421-27. [PMID: 22487585]
Smith D. K., Switzer W. M., Peters P., et al. A strategy for PrEP clinicians to manage ambiguous HIV test results during follow-up visits. Open Forum Infect Dis 2018;5(8):ofy180. [PMID: 30568989]
Spinelli M. A., Glidden D. V., Anderson P. L., et al. Impact of estimated pre-exposure prophylaxis (PrEP) adherence patterns on bone mineral density in a large PrEP demonstration project. AIDS Res Hum Retroviruses 2019;35(9):788-93. [PMID: 31119944]
Stewart J., Oware K., Donnell D., et al. Doxycycline prophylaxis to prevent sexually transmitted Infections in women. N Engl J Med 2023;389(25):2331-40. [PMID: 38118022]
Tang E. C., Vittinghoff E., Philip S. S., et al. Quarterly screening optimizes detection of sexually transmitted infections when prescribing HIV preexposure prophylaxis. AIDS 2020;34(8):1181-86. [PMID: 32205724]
Taylor D., Lunny C., Wong T., et al. Self-collected versus clinician-collected sampling for sexually transmitted infections: a systematic review and meta-analysis protocol. Syst Rev 2013;2(1):93. [PMID: 24112441]
Thigpen M. C., Kebaabetswe P. M., Paxton L. A., et al. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med 2012;367(5):423-34. [PMID: 22784038]
Thomson K. A., Hughes J., Baeten J. M., et al. Increased risk of HIV acquisition among women throughout pregnancy and during the postpartum period: a prospective per-coital-act analysis among women with HIV-infected partners. J Infect Dis 2018;218(1):16-25. [PMID: 29514254]
Tolley E. E., Zangeneh S. Z., Chau G., et al. Acceptability of long-acting injectable cabotegravir (CAB LA) in HIV-uninfected individuals: HPTN 077. AIDS Behav 2020;24(9):2520-31. [PMID: 32052214]
Townes A.R., Tanner M., Henry K.D., et al. Low proportions of linkage & prescriptions of PrEP in Black women (THRIVE, 2015-2020). CROI; 2021 Mar 6-10; Virtual. https://www.croiconference.org/abstract/low-proportions-of-linkage-prescriptions-of-prep-in-black-women-thrive-2015-2020/
USPSTF. Preexposure prophylaxis to prevent acquisition of HIV: US Preventive Services Task Force recommendation statement. JAMA 2023;330(8):736-45. [PMID: 37606666]
Van Damme L., Corneli A., Ahmed K., et al. Preexposure prophylaxis for HIV infection among African women. N Engl J Med 2012;367(5):411-22. [PMID: 22784040]
van de Vijver D. A., Mukherjee S., van Kampen J.J. Antiretroviral drug treatment of individuals that used preexposure prophylaxis (PrEP) before diagnosis. Curr Treat Options Infect Dis 2021;13:141-52. https://doi.org/10.1007/s40506-021-00246-9
van der Sluis W. B., Bouman M. B., Gijs L., et al. Gonorrhoea of the sigmoid neovagina in a male-to-female transgender. Int J STD AIDS 2015;26(8):595-98. [PMID: 25060698]
Vanhommerig J. W., Lambers F. A., Schinkel J., et al. Risk factors for sexual transmission of hepatitis C virus among human immunodeficiency virus-infected men who have sex with men: a case-control study. Open Forum Infect Dis 2015;2(3):ofv115. [PMID: 26634219]
Vernazza P. L., Graf I., Sonnenberg-Schwan U., et al. Preexposure prophylaxis and timed intercourse for HIV-discordant couples willing to conceive a child. AIDS 2011;25(16):2005-8. [PMID: 21716070]
Vigano A., Mora S., Giacomet V., et al. In utero exposure to tenofovir disoproxil fumarate does not impair growth and bone health in HIV-uninfected children born to HIV-infected mothers. Antivir Ther 2011;16(8):1259-66. [PMID: 22155907]
Walters S. M., Coston B., Neaigus A., et al. The role of syringe exchange programs and sexual identity in awareness of pre-exposure prophylaxis (PrEP) for male persons who inject drugs. Int J Drug Policy 2020;77:102671. [PMID: 32092665]
Wen W. H., Chen H. L., Shih T. T., et al. Long-term growth and bone development in children of HBV-infected mothers with and without fetal exposure to tenofovir disoproxil fumarate. J Hepatol 2020;72(6):1082-87. [PMID: 32044401]
Whelchel K., Zuckerman A. D., DeClercq J., et al. Optimizing HIV PrEP persistence: does your pharmacy matter?. AIDS Behav 2023;27(11):3735-44. [PMID: 37266824]
Williams E., Williamson D. A., Hocking J. S. Frequent screening for asymptomatic chlamydia and gonorrhoea infections in men who have sex with men: time to re-evaluate?. Lancet Infect Dis 2023;23(12):e558-66. [PMID: 37516129]
Workowski K. A., Bolan G. A. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep 2015;64(RR-03):1-137. [PMID: 26042815]
Yager J., Brooks K. M., Brothers J., et al. Gender-affirming hormone pharmacokinetics among adolescent and young adult transgender persons receiving daily emtricitabine/tenofovir disoproxil fumarate. AIDS Res Hum Retroviruses 2022;38(12):939-43. [PMID: 35815468]
Zeng Q. L., Zhou Y. H., Dong X. P., et al. Expected 8-week prenatal vs 12-week perinatal tenofovir alafenamide prophylaxis to prevent mother-to-child transmission of hepatitis B virus: a multicenter, prospective, open-label, randomized controlled trial. Am J Gastroenterol 2025;120(5):1045-56. [PMID: 39382852]
Zetola N. M., Bernstein K. T., Wong E., et al. Exploring the relationship between sexually transmitted diseases and HIV acquisition by using different study designs. J Acquir Immune Defic Syndr 2009;50(5):546-51. [PMID: 19367993]
Zucker J., Carnevale C., Rai A. J., et al. Positive or not, that is the question: HIV testing for individuals on pre-exposure prophylaxis. J Acquir Immune Defic Syndr 2018;78(2):e11-13. [PMID: 29481487]
Zule W. A., Costenbader E. C., Meyer W. J., et al. Methamphetamine use and risky sexual behaviors during heterosexual encounters. Sex Transm Dis 2007;34(9):689-94. [PMID: 17471112]
Updates, Authorship, and Related Guidelines
| Updates, Authorship, and Related Guidelines | |
| Date of original publication | October 10, 2019 |
| Date of current publication | October 16, 2025 |
| Highlights of changes, additions, and updates in the October 16, 2025 edition |
|
| Intended users | Clinicians recommending, initiating, or maintaining PrEP care for individuals at risk of acquiring HIV |
| Lead author(s) |
Rona M. Vail, MD, AAHIVS; Aviva Cantor, DMSc, PA, AAHIVS |
| Writing group |
Sanjiv S. Shah, MD, MPH, AAHIVS; Steven M. Fine, MD, PhD; Joseph P. McGowan, MD, FACP, FIDSA, AAHIVS; Samuel T. Merrick, MD, FIDSA; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Anne K. Monroe, MD, MSPH; Jessica Rodrigues, MPH, MS; Christopher J. Hoffmann, MD, MPH, MSc, FACP; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD |
| Author and writing group conflict of interest disclosures | There are no author or writing group conflict of interest disclosures. |
| Committee | |
| Developer and funder |
New York State Department of Health AIDS Institute (NYSDOH AI) |
| Development process |
See Guideline Development and Recommendation Ratings Scheme, below. |
| Related NYSDOH AI guidelines |
Guidelines
Guidance
Podcast |
Guideline Development and Recommendation Ratings
| Guideline Development: New York State Department of Health AIDS Institute Clinical Guidelines Program | |
| Program manager | Clinical Guidelines Program, Johns Hopkins University School of Medicine, Division of Infectious Diseases. See Program Leadership and Staff. |
| Mission | To produce and disseminate evidence-based, state-of-the-art clinical practice guidelines that establish uniform standards of care for practitioners who provide prevention or treatment of HIV, viral hepatitis, other sexually transmitted infections, and substance use disorders for adults throughout New York State in the wide array of settings in which those services are delivered. |
| Expert committees | The NYSDOH AI Medical Director invites and appoints committees of clinical and public health experts from throughout New York State to ensure that the guidelines are practical, immediately applicable, and meet the needs of care providers and stakeholders in all major regions of New York State, all relevant clinical practice settings, key New York State agencies, and community service organizations. |
| Committee structure |
|
| Disclosure and management of conflicts of interest |
|
| Evidence collection and review |
|
| Recommendation development |
|
| Review and approval process |
|
| External reviews |
|
| Update process |
|
| Recommendation Ratings Scheme | |||
| Strength | Quality of Evidence | ||
| Rating | Definition | Rating | Definition |
| A | Strong | 1 | Based on published results of at least 1 randomized clinical trial with clinical outcomes or validated laboratory endpoints. |
| B | Moderate | * | Based on either a self-evident conclusion; conclusive, published, in vitro data; or well-established practice that cannot be tested because ethics would preclude a clinical trial. |
| C | Optional | 2 | Based on published results of at least 1 well-designed, nonrandomized clinical trial or observational cohort study with long-term clinical outcomes. |
| 2† | Extrapolated from published results of well-designed studies (including nonrandomized clinical trials) conducted in populations other than those specifically addressed by a recommendation. The source(s) of the extrapolated evidence and the rationale for the extrapolation are provided in the guideline text. One example would be results of studies conducted predominantly in a subpopulation (e.g., one gender) that the committee determines to be generalizable to the population under consideration in the guideline. | ||
| 3 | Based on committee expert opinion, with rationale provided in the guideline text. | ||
Last updated on May 12, 2026