
Purpose of This Guideline
Date of current publication: September 25, 2023
Lead authors: Daniela E. DiMarco, MD, MPH; Marguerite A. Urban, MD
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Joseph P. McGowan, MD, FACP, FIDSA; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Jessica Rodrigues, MS; Charles J. Gonzalez, MD; Christopher J. Hoffmann, MD, MPH
Committee: Medical Care Criteria Committee
Date of original publication: September 25, 2023
This guideline on the use of doxycycline post-exposure prophylaxis (doxy-PEP) for prevention of bacterial sexually transmitted infections (STIs), including syphilis, chlamydia, and gonorrhea, was developed by the New York State Department of Health AIDS Institute (NYSDOH AI) Clinical Guidelines Program to support clinicians in caring for adults and adolescents with and without HIV who are at risk of STIs. The goals of this guideline are to:
- Summarize the available evidence regarding the use of doxy-PEP for preventing syphilis, chlamydia, and gonorrhea infections
- Provide evidence-based clinical recommendations for the use of doxy-PEP
- Present practical considerations for prescribing doxy-PEP
The literature on this topic is evolving rapidly, with several clinical trials ongoing. To prepare this guideline, the authors conducted a review of the published literature through MEDLINE, conference presentations, and existing published guidance within the United States and internationally.
Biomedical Prevention of STIs
| RECOMMENDATIONS |
Biomedical Prevention of STIs
|
Abbreviations: doxy-PEP, doxycycline post-exposure prophylaxis; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection. |
The United States, including New York State, continues to see high rates of reportable STIs, specifically syphilis, chlamydia, and gonorrhea, despite decades of public health efforts and prevention strategies aimed at curbing the STI epidemic. Except for the year 2020, in which there was an interruption of in-person care and STI testing related to the COVID-19 pandemic, rates of these reportable STIs have steadily increased since 2015, with some populations disproportionately affected, including men who have sex with men (MSM), young people, and some racial and ethnic minority groups CDC 2023. The most recent (2021) STI surveillance data from the Centers for Disease Control and Prevention (CDC) note that reportable STIs continue to disproportionately impact people who identify as Black/African American and American Indian/Alaska Native CDC 2023, making clear that established STI prevention strategies are insufficient.
Biomedical methods for HIV prevention with HIV PrEP and PEP have been very effective. Researchers identified doxycycline as a candidate for biomedical prevention of STIs. In 2011, Wilson and colleagues used mathematical modeling based on sexual behavior factors to predict doxy-PEP efficacy among MSM in Australia. Assuming 50% uptake and 70% efficacy, the model predicted a 50% reduction in syphilis cases after 1 year and an 85% reduction after 10 years Wilson, et al. 2011. Doxycycline is an antibiotic in the tetracycline class approved by the U.S. Food and Drug Administration for the management of many different types of infections Lexicomp 2023; FDA 2016. Doxycycline is available in 2 different formulations: hyclate, which is more water soluble, and monohydrate, which is less water soluble so may have fewer gastrointestinal adverse effects. Common uses include treatment of chlamydia, syphilis, respiratory infections, and skin and soft tissue infections. Doxycycline has also been used as both a PrEP and PEP agent for certain bacterial and parasitic infections, including Lyme disease, leptospirosis, and malaria Grant, et al. 2020. When used in nonpregnant adults, doxycycline is safe and well tolerated, has excellent oral bioavailability, is low cost, and is widely available. Adverse effects of doxycycline are generally mild, with gastrointestinal symptoms being the most common. Other adverse effects include photosensitivity and esophageal injury. Doxycycline is contraindicated in pregnancy because of potential adverse effects on the fetus Lexicomp 2023. Doxycycline is also used safely for prolonged periods for some conditions, including acne Zaenglein, et al. 2016 and prosthetic joint infections Osmon, et al. 2013. These factors make doxycycline a promising prophylactic agent; however, the effects on antimicrobial resistance and the microbiome with widespread use are still under investigation.
Acceptability of Doxycycline for STI Prophylaxis
Several surveys conducted among MSM with STI risk factors have demonstrated interest in and acceptability of a biomedical STI prevention option Fusca, et al. 2020; Spinelli, et al. 2019; Wilson, et al. 2011. An online survey in Southern California of 212 community members identifying as MSM and 76 healthcare providers found that acceptance of doxycycline as PEP or PrEP was greater among community members taking HIV PrEP or with a recent STI diagnosis than it was among those not taking HIV PrEP or without a recent STI diagnosis Park, et al. 2021. For healthcare providers, a recommendation from the CDC was associated with significantly greater willingness to prescribe doxy-PEP/PrEP. All respondents expressed concern regarding antibiotic resistance Park, et al. 2021. In the DoxyPEP study reviewed below, acceptability of doxy-PEP was 88% in the study population of cisgender men and transgender women who have sex with men Luetkemeyer, et al. 2023.
Surveys conducted in the United Kingdom, the Netherlands, and Australia found that in the absence of established guidelines, antibiotics including doxycycline were being used off-label for STI prophylaxis, particularly by individuals taking HIV PrEP O'Halloran, et al. 2021; Evers, et al. 2020; Chow and Fairley 2019; Carveth-Johnson, et al. 2018, demonstrating a need for further investigation to guide evidence-based use of doxycycline prophylaxis.
To facilitate shared decision-making with patients, it is important that clinicians are aware of the indications for and how to prescribe and manage doxy-PEP and become familiar with the benefits, risks, and limitations surrounding its use.
Doxycycline as PEP
Available evidence on doxycycline prophylaxis to prevent bacterial STIs is limited but increasing. Current data are from randomized clinical trials, observational studies, modeling studies, and surveys on acceptability for use. Studies predominantly included cisgender men and transgender women who have sex with men who were receiving HIV PrEP or in care for HIV infection, were aged 35 years and older, and were White.
In 4 randomized clinical trials comparing doxy-PEP with standard of care (routine STI testing), participants received HIV PrEP or HIV care, and in 3 of the 4 trials participants had a history of ≥1 bacterial STI in the prior year. The study protocols used a 200 mg dose of oral doxycycline taken ideally within 24 hours or up to 72 hours of condomless sex to prevent bacterial STIs. All participants were tested for STIs every 3 months during the study period Luetkemeyer, et al. 2023; Molina, et al. 2023; Stewart, et al. 2023; Molina, et al. 2018. In the 3 trials conducted among cisgender men and transgender women who have sex with men, there were significant reductions in chlamydia and syphilis, but results were mixed regarding the efficacy of doxy-PEP in preventing gonococcal infection, likely at least in part due to geographic variability in prevalence of tetracycline resistance in gonococci Luetkemeyer, et al. 2023; Molina, et al. 2023; Fairley and Chow 2018; Molina, et al. 2018; Siguier and Molina 2018. In a study that included only cisgender women taking HIV PrEP, doxy-PEP was not effective at preventing bacterial STIs Stewart, et al. 2023.
A modeling study analyzed data from an LGBTQ-focused health center in the United States to assess the effect of doxy-PEP use on STI incidence among more than 10,000 individuals assigned male sex at birth (including cisgender men, transgender women, and nonbinary individuals) who had male sex partners and STI testing (chlamydia, gonorrhea, or syphilis) on record Traeger, et al. 2023. STI incidence was 35.9 per 100 person-years. Modeling demonstrated that, rather than prescribing doxy-PEP based solely on HIV or PrEP engagement, prescribing based on STI history resulted in an efficient strategy that balanced uptake and preventive impact. An approach combining these factors, as was done in the clinical trials, was not modeled in this projection. Seven different strategies for prescribing doxy-PEP over 12 months were modeled. Prescribing to all in the sample, an estimated 71% of gonorrhea, chlamydia, and syphilis cases could have been averted, with a number needed to treat (NNT) of 3.9. Prescribing to individuals with HIV (12%) or who were taking HIV PrEP (52%) could have averted 60% of STI diagnoses in this group, with an NNT of 2.9. With prescribing limited to individuals with an STI diagnosis, the proportion using doxy-PEP was reduced to 38% and would have averted 39% of STI diagnoses, with an NNT of 2.4.
This committee’s recommendations on provision of doxy-PEP are outlined above, and implementation considerations are discussed in the guideline section Practical Considerations for Doxy-PEP Implementation. The eligibility criteria for doxy-PEP use include a history of a bacterial STI in the prior year as was done in the existing research trials. However, other factors are associated with increased risk of STI exposure, including engaging in group sex, engaging in transactional sex, and combining sex and substance use Workowski, et al. 2021. An STI risk assessment is an individualized process, and the risk-benefit profile for doxy-PEP is expected to vary based on individual patient factors and community and sexual network prevalence. This individualized assessment is an important aspect of the shared decision-making between patient and clinician.
The recommendation for doxy-PEP use among cisgender men and transgender women who have sex with men is based on the significant reductions in bacterial STIs reported in the 3 clinical trials described in detail below. Although the majority of STIs among these populations are asymptomatic and without complications, the significant decrease in STI occurrence provides potential benefits to individuals and the broader community and likely outweighs the potential harms of doxycycline use. Based on the lack of efficacy reported for doxy-PEP in cisgender women in Kenya Stewart, et al. 2023, doxy-PEP is not recommended for use in individuals at risk of STIs through receptive vaginal sex, despite pharmacologic data from an unrelated study suggesting adequate tissue and secretion levels for protection Haaland, et al. 2023.
There are no data evaluating doxy-PEP use among cisgender men with sex partners assigned female sex at birth. However, doxy-PEP use among cisgender men (with female partners) who have similar STI risk factors as the doxy-PEP study populations (i.e., history of STIs, multiple sex partners, high-prevalence populations) could also potentially provide individual and community benefits outweighing the risks of doxycycline use. The NNT and degree of potential protective effect with insertive vaginal sex are unknown. This strategy has the possibility of extending the potential benefits of doxy-PEP use, indirectly, to cisgender women (who have sex with men) and neonates who experience the majority of complications of bacterial STIs through reduction of community rates and may be considered by clinicians on a case-by-case basis. Doxy-PEP has not been studied in adolescents <18 years old, so adherence and efficacy in this group are unknown.
Evidence from the IPERGAY trial: The first published evidence on doxy-PEP was derived from a substudy of the ANRS IPERGAY randomized trial of on-demand HIV PrEP among cisgender men and transgender women who have sex with men in France, which demonstrated an approximately 70% reduction in incident chlamydia and syphilis infections but no significant reduction in gonorrhea infections in a population reporting sex practices placing them at high risk of STIs Molina, et al. 2018. In this open-label extension, more than 200 participants (cisgender men and transgender women who have sex with men) taking HIV PrEP were randomized to receive doxycycline hyclate 200 mg as a single dose within 24 to 72 hours after condomless sex or no doxy-PEP Molina, et al. 2018. Study participants were mostly White, >30 years old, and reported having multiple sex partners (10 in 2 months) and engaging in condomless sex acts (10 in 4 weeks). Participants were instructed not to exceed 3 doses per week; the median number of doxy-PEP doses used per month was 3.4, which was fewer than the number of reported condomless sexual encounters. Of participants, 83% took doxy-PEP within 24 hours of sex. Gastrointestinal adverse effects were reported by more than half of the participants, resulting in 8 discontinuations. Doxy-PEP was associated with significant reductions in the incidence of first STI and, in individual analyses, of incident chlamydia and syphilis infections. For incident gonorrhea, however, there was no significant reduction in the doxy-PEP group, which was attributed to the high prevalence of tetracycline resistance among gonococcal isolates in France Molina, et al. 2018.
Evidence from the DoxyPEP trial: The open-label randomized DoxyPEP study analyzed data from 501 adult cisgender MSM (96%) and transgender women who have sex with men (4%) who were either taking HIV PrEP (n=360) or had HIV (n=194) and who had a bacterial STI and reported condomless sex with a male partner within the past year. Participants were randomized to receive either doxy-PEP as 200 mg of delayed-release doxycycline hyclate (ideally within 24 hours but no later than 72 hours after condomless sex) or standard of care Luetkemeyer, et al. 2023. STI testing was performed every 3 months over 1 year of follow-up. Participants had a high prevalence of baseline bacterial STIs and a median of 9 sex partners in the 3 months before enrollment, and 59% reported substance use. The median participant age was 38 years, and more than 67% were White, 7% were Black, 11% were Asian or Pacific Islander, 15% were multiracial or other, and 30% were Hispanic. The maximum dose of doxycycline was 200 mg within a 24-hour period, and the medication was dispensed at 3-month intervals. The initial doxycycline supply included enough tablets for daily use, and the amount dispensed each quarter was adjusted in follow-up based on frequency of sex and doses used.
The DoxyPEP study was stopped early after interim analysis noted a significant protective effect in the intervention arm, and participants in the standard-of-care group were offered doxy-PEP Luetkemeyer, et al. 2023. Modified intention-to-treat analysis included participants who completed a median of 9 months of follow-up Luetkemeyer, et al. 2023. Gonorrhea was the most common STI diagnosed, and there were very few cases of early syphilis. Median doxy-PEP use was 4 doses per month, with 25% of participants reporting more than 10 doses per month. This study demonstrated a 52% quarterly reduction in any incident STI among participants with HIV (hazard ratio [HR], 0.48; 95% confidence interval [CI], 0.28-0.83), and a 66% reduction among those taking HIV PrEP (HR, 0.34; 95% CI, 0.23-0.51) Luetkemeyer, et al. 2023; Luetkemeyer, et al. 2022; SFDPH 2022. Among participants taking HIV PrEP, the relative risk (RR) of any incident STI was 0.34 (95% CI, 0.24-0.46; P<.001), and the NNT was 4.7, whereas among participants with HIV, the RR for any incident STI was 0.38 (95% CI, 0.24-0.60; P<.001), and the NNT was 5.3.
In subgroup analyses, among participants taking HIV PrEP, the significant risk reduction was maintained for each STI individually, including infections at extragenital sites, except for pharyngeal chlamydia Luetkemeyer, et al. 2023. Among participants with HIV, doxy-PEP did not significantly reduce incident early syphilis or urethral or pharyngeal chlamydia or gonorrhea. Doxycycline was well tolerated, and self-reported adherence was high. Antimicrobial resistance was also evaluated in this study and is discussed below (see guideline section Antimicrobial Resistance, below).
Evidence from the DOXYVAC trial: In the phase III randomized 2×2 factorial designed DOXYVAC trial, the efficacy of both doxy-PEP for bacterial STI prophylaxis and meningococcal serotype B vaccination for preventing gonococcal infection was investigated among 446 cisgender men and transgender women who have sex with men taking HIV PrEP in France Molina, et al. 2023. Participants were predominantly White, had a median age of 39 years, were long-term HIV PrEP users, reported multiple sex partners, and had multiple prior STIs. Unblinded early interim analysis revealed significant reductions in any incident STI, and participants were all offered doxy-PEP. Doxy-PEP significantly reduced the incidence of the first episode of chlamydia (adjusted HR [aHR], 0.11; 95% CI, 0.04-0.30; P<.0001), syphilis (aHR, 0.21; 95% CI, 0.09-0.47; P<.001), gonorrhea (aHR, 0.49; 95% CI, 0.32-0.76; P<.001), and Mycoplasma genitalium (aHR, 0.55; 95% CI, 0.34-0.89; P=.015) infections. Adherence was also high in this study at approximately 80%, with a median use of 3.5 doses per month and a median time to doxy-PEP intake after sex of 27 hours. Additionally, antimicrobial resistance was analyzed and is discussed below (see guideline section Antimicrobial Resistance, below).
Doxy-PEP and receptive vaginal sex: Preliminary data from a randomized trial in Kisumu, Kenya, that compared doxy-PEP with the standard of care among cisgender women who were 18 to 30 years old and taking HIV PrEP found that doxy-PEP was not effective for bacterial STI prevention in this population Stewart, et al. 2023. The study enrolled 449 participants from 2020 to 2022, with very little loss to follow-up. At baseline, 18% of participants were diagnosed with an STI (14% with chlamydia, 4% with gonorrhea, and <1% with syphilis). Data on doxy-PEP adherence were self-reported, with 78% of condomless sex encounters covered. Incident STIs were similar between groups (annual incidence of 27%), with no significant reduction in the doxy-PEP group. No incident HIV infections were reported. The reason for the lack of demonstrable efficacy of doxy-PEP in this study is unclear. Possible factors influencing these results include the prevalence of high-level tetracycline resistance among gonococcal isolates in Kenya Soge, et al. 2023, adherence being less than what was ascertained by self-report, and biologic or anatomic differences. An unrelated study in the United States evaluated drug concentrations with event-driven oral dosing and showed that 200 mg of doxycycline hyclate achieved concentrations above minimum inhibitory concentrations (MICs) for syphilis, chlamydia, and gonorrhea in rectal, vaginal, and cervical tissues as well as rectal and vaginal secretions; these concentrations were sustained at least 2 days after dosing, although the degree above MIC was much lower for Neisseria gonorrhoeae Haaland, et al. 2023. Higher doxycycline concentrations were sustained for a longer duration in rectal secretions than in vaginal secretions, although the levels remained above the MIC.
Doxy-PEP has not been studied in gender-diverse populations at risk of STIs through receptive vaginal sex.
| KEY POINTS |
|
Antimicrobial Resistance
Published research, previous guideline statements, and editorials have raised concerns about the impact of doxy-PEP on the emergence of antimicrobial resistance for bacterial STIs and other non-STI pathogens with widespread long-term use Cornelisse, et al. 2023; Luetkemeyer, et al. 2023; Molina, et al. 2023; Kohli, et al. 2022; Lewis 2022; Luetkemeyer, et al. 2022; Grant, et al. 2020; Molina, et al. 2018; Siguier and Molina 2018; Golden and Handsfield 2015. Increasing antimicrobial resistance is a concern at both the individual and population levels Cornelisse, et al. 2023. It may take years to determine this effect, and additional research is needed Siguier and Molina 2018. To date, studies of doxy-PEP have not found detectable resistance in Treponema pallidum or Chlamydia trachomatis strains Cornelisse, et al. 2023. Doxycycline resistance is already a concern for other bacterial STIs, including M. genitalium and N. gonorrhoeae, and there are few alternative therapeutic options for M. genitalium Workowski, et al. 2021. Tetracycline (used as a surrogate for doxycycline) resistance in N. gonorrhoeae isolates varies geographically and is reported at 20.6% nationwide by the CDC Gonococcal Isolate Surveillance Project CDC 2023. Doxycycline is an important antibiotic used to treat non-sexually transmitted infections when other oral treatment options are severely limited, including methicillin-resistant Staphylococcus aureus (MRSA). Doxycycline also remains an option for antimicrobial-resistant gonococcal infections if susceptibility is confirmed. The benefits of widespread use of doxycycline must be weighed against the known and potential risks of selecting for antimicrobial resistance and altering the various microbiomes (e.g., gastrointestinal, vaginal, skin). In an analysis of more than 2,000 gonococcal isolates in Europe, the presence of 2 common tetracycline-associated mutations was strongly associated with additional mutations conferring cross-resistance to other antibiotics, including beta-lactams, macrolides, and fluoroquinolones Vanbaelen, et al. 2023. This raises concern that selecting for gonorrhea tetracycline resistance may also impact the effectiveness of other antibiotic classes, including cephalosporins, which are the standard of care for gonorrhea treatment.
To assess the impact of doxy-PEP use on antimicrobial resistance, nares and oropharynx specimens were examined for S. aureus in the DoxyPEP study Luetkemeyer, et al. 2023, and tetracycline resistance in extended-spectrum beta-lactamase (ESBL) Escherichia coli (as a marker of microbiome influence) and MRSA were assessed in the DOXYVAC study Molina, et al. 2023. In the DoxyPEP study, cultures were available for 17.2% of gonorrhea infections (n=44) Luetkemeyer, et al. 2023. Of these, baseline tetracycline resistance (a surrogate for doxycycline resistance) was 27%. After enrollment, resistance was 38% in the doxycycline groups and 12% in the standard-of-care groups, and doxy-PEP appeared less protective for tetracycline-resistant gonorrhea, although the sample size was small Luetkemeyer, et al. 2023; Luetkemeyer, et al. 2022. S. aureus was cultured from the oronasopharynx in 45% of participants, and baseline doxycycline resistance was 12% Luetkemeyer, et al. 2023. At 1 year, S. aureus colonization identified by culture was significantly less in the doxy-PEP groups than the standard-of-care groups, and prevalence of doxycycline-resistant isolates was 16% in the doxycycline groups and 8% in the standard-of-care groups Luetkemeyer, et al. 2023. In the DOXYVAC study, cultures were available for 15% of gonorrhea infections Molina, et al. 2023. Baseline tetracycline resistance was 100%, and the prevalence of high-level resistance was greater in the doxy-PEP group (33.3%) than in the standard-of-care group (18.9%). As markers for assessing the impact of doxy-PEP on the microbiome, there was no significant difference in detection of ESBL E. coli from anal swabs or MRSA from the pharynx.
Based on these data, the efficacy of doxy-PEP for gonorrhea is expected to differ depending on the prevalence of tetracycline resistance in a given population or geographic region. For S. aureus, doxy-PEP is associated with increased resistance Luetkemeyer, et al. 2023, which is an important consideration in the preservation of antimicrobial treatment options for MRSA infection.
Recommendations Outside of New York State
Several organizations have issued guidance regarding the use of doxy-PEP CDC 2023; CDPH 2023; Cornelisse, et al. 2023; Gandhi, et al. 2023; NCSD 2023; PHSKC 2023; SCPHD 2023; Kohli, et al. 2022; SFDPH 2022. There is significant variability regarding implementation of this intervention, although dosing recommendations have been uniformly consistent with the dosing used in the studies to date.
United Kingdom and Australian guidelines did not recommend doxy-PEP implementation Cornelisse, et al. 2023; Kohli, et al. 2022, but position statements have summarized the available evidence (including risks and benefits) to provide some clinical guidance when patients are seeking or already taking doxycycline prophylaxis. The British Association for Sexual Health and HIV and the UK Health Security Agency do not endorse the use of doxycycline as prophylaxis, primarily because of concerns regarding antimicrobial resistance and limited long-term data Kohli, et al. 2022. The Australian Society for HIV, Viral Hepatitis, and Sexual Health Medicine does not recommend for or against doxy-PEP but advises clinicians to consider the risks and benefits at the individual and population levels, with a focused discussion of concerns with widespread use including the potential for selection of antimicrobial resistance and impact on the microbiome Cornelisse, et al. 2023.
At the time of this writing, the CDC has not formally recommended for or against doxycycline use for bacterial STI prophylaxis CDC 2023. In 2022, based on preliminary data from the DoxyPEP study, the CDC updated its STI treatment guidelines to include a brief summary of the available evidence on doxy-PEP and recommend that, if prescribed as PEP, 200 mg of oral doxycycline be taken within 24 to 72 hours after sex (as in the DoxyPEP study protocol) and that patients be provided with education and counseling regarding the risks CDC 2023. In their 2022 recommendations, the International Antiviral Society-USA recommended that until more data are available, doxy-PEP should be considered on a case-by-case basis for individuals at elevated risk of these bacterial STIs Gandhi, et al. 2023.
The San Francisco Department of Public Health (SFDPH) released implementation guidance in October 2022 recommending doxy-PEP for cisgender men and transgender women who meet 2 eligibility criteria outlined in the DoxyPEP study: 1) have a diagnosis of a bacterial STI within the last year, and 2) report condomless sex with at least 1 male partner in the past year SFDPH 2022. The SFDPH also recommends offering doxy-PEP via shared decision-making to cisgender men, transgender men, and transgender women who have had multiple sex partners assigned male sex at birth within the past year, even in the absence of a prior STI diagnosis. Additionally, the SFDPH recommends comprehensive sexual health services that include routine STI testing, and counseling patients on the known and potential effects of doxy-PEP use on antimicrobial resistance and the microbiome, efficacy data on and limitations of doxy-PEP, and potential adverse effects. The SFDPH dosing and prescribing recommendations are the same as those used in the DoxyPEP study; however, the SFDPH notes that immediate- or extended-release doxycycline could be used, although the extended-release formulation may be more expensive. The California Department of Health (CDPH) sent out a Dear Colleague Letter on April 28, 2023, with recommendations on doxy-PEP CDPH 2023. The CDPH recommends doxy-PEP for cisgender men or transgender women with ≥1 bacterial STI in the past 12 months and suggests offering doxy-PEP via shared decision-making to all nonpregnant individuals at increased risk of STI acquisition, even if there is no history of an STI diagnosis. Similar to San Francisco, the CDPH also recommends including comprehensive sexual health counseling and education.
In June 2023, the King County Sexual Health Clinic in Seattle, Washington, released doxy-PEP guidelines recommending that clinicians engage in shared decision-making on doxy-PEP with cisgender men and transgender women with history of an STI in the past year and ongoing sex encounters with partners assigned male sex at birth PHSKC 2023. Their guidance recommends stronger consideration for those in this population with a specific history of syphilis or multiple STIs in the prior year, and also that clinicians may consider prescribing doxy-PEP episodically when patients anticipate their STI exposure risk to be elevated (using group sex events as an example).
The National Coalition of STD Directors released a doxy-PEP implementation toolkit with basic guidance on community engagement, workflow, education, program evaluation, and prescribing logistics NCSD 2023. Highlights from the toolkit emphasize ensuring equitable criteria for offering doxy-PEP and reducing unnecessary access restrictions.
Practical Considerations for Doxy-PEP Implementation
As with any drug therapy, a review of the patient’s health history, current medications, and allergies to ensure there are no health concerns, drug-drug interactions, or medication allergies that would preclude use is indicated before initiating doxycycline post-exposure prophylaxis (doxy-PEP). Concurrent use of doxy-PEP with daily doxycycline or tetracycline for other conditions is contraindicated. Medications other than doxycycline have not been studied for bacterial sexually transmitted infection (STI) PEP. When doxycycline is not tolerated or contraindications to its use exist, doxy-PEP is not recommended. Practical considerations for prescribing and monitoring doxy-PEP are outlined in Table 1, below.
| Abbreviations: ARV, antiretroviral medication; BUN, blood urea nitrogen; CBC, complete blood count; doxy-PEP, doxycycline post-exposure prophylaxis; GI, gastrointestinal; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection.
Notes:
|
|
| Table 1: Considerations for Doxy-PEP Implementation | |
| Consideration(s) | Comments |
| Available formulations |
|
| Administration |
|
| Contraindications, drug-drug interactions, and dose adjustments |
|
| Adverse effects |
|
| Supply of doxy-PEP medications |
|
| Follow-up and laboratory monitoring |
|
| Key points for patient education |
|
Download Table 1: Considerations for Doxy-PEP Implementation Printable PDF
Treat any patient diagnosed with gonorrhea, chlamydia, or syphilis while taking doxy-PEP according to the Centers for Disease Control and Prevention (CDC) STI Treatment Guidelines Workowski, et al. 2021.
For patients taking doxy-PEP who present for care after a sexual partner(s) is diagnosed with chlamydia or gonorrhea, a clinical evaluation that includes STI testing with a shared decision-making approach regarding presumptive treatment is the suggested approach. Acknowledging that doxy-PEP is not 100% effective, CDC guidance recommends presumptive treatment for patients exposed to chlamydia or gonorrhea within the past 60 days, regardless of test results Workowski, et al. 2021. An alternative option for those who decline presumptive treatment is to administer treatment based on test results and continue STI screening every 3 months.
Patients taking doxy-PEP who are exposed to early syphilis within the prior 90 days can also be treated presumptively per the CDC STI Treatment Guidelines Workowski, et al. 2021 regardless of test results. If treatment is declined, repeat syphilis testing at 3 months is necessary due to the potential for an extended period of syphilis incubation.
All Recommendations
| ALL RECOMMENDATIONS: DOXYCYCLINE POST-EXPOSURE PROPHYLAXIS TO PREVENT BACTERIAL SEXUALLY TRANSMITTED INFECTIONS |
Biomedical Prevention of STIs
|
Abbreviations: doxy-PEP, doxycycline post-exposure prophylaxis; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection. |
Shared Decision-Making
Download Printable PDF of Shared Decision-Making Statement
Date of current publication: August 8, 2023
Lead authors: Jessica Rodrigues, MS; Jessica M. Atrio, MD, MSc; and Johanna L. Gribble, MA
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: August 8, 2023
Rationale
Throughout its guidelines, the New York State Department of Health (NYSDOH) AIDS Institute (AI) Clinical Guidelines Program recommends “shared decision-making,” an individualized process central to patient-centered care. With shared decision-making, clinicians and patients engage in meaningful dialogue to arrive at an informed, collaborative decision about a patient’s health, care, and treatment planning. The approach to shared decision-making described here applies to recommendations included in all program guidelines. The included elements are drawn from a comprehensive review of multiple sources and similar attempts to define shared decision-making, including the Institute of Medicine’s original description [Institute of Medicine 2001]. For more information, a variety of informative resources and suggested readings are included at the end of the discussion.
Benefits
The benefits to patients that have been associated with a shared decision-making approach include:
- Decreased anxiety [Niburski, et al. 2020; Stalnikowicz and Brezis 2020]
- Increased trust in clinicians [Acree, et al. 2020; Groot, et al. 2020; Stalnikowicz and Brezis 2020]
- Improved engagement in preventive care [McNulty, et al. 2022; Scalia, et al. 2022; Bertakis and Azari 2011]
- Improved treatment adherence, clinical outcomes, and satisfaction with care [Crawford, et al. 2021; Bertakis and Azari 2011; Robinson, et al. 2008]
- Increased knowledge, confidence, empowerment, and self-efficacy [Chen, et al. 2021; Coronado-Vázquez, et al. 2020; Niburski, et al. 2020]
Approach
Collaborative care: Shared decision-making is an approach to healthcare delivery that respects a patient’s autonomy in responding to a clinician’s recommendations and facilitates dynamic, personalized, and collaborative care. Through this process, a clinician engages a patient in an open and respectful dialogue to elicit the patient’s knowledge, experience, healthcare goals, daily routine, lifestyle, support system, cultural and personal identity, and attitudes toward behavior, treatment, and risk. With this information and the clinician’s clinical expertise, the patient and clinician can collaborate to identify, evaluate, and choose from among available healthcare options [Coulter and Collins 2011]. This process emphasizes the importance of a patient’s values, preferences, needs, social context, and lived experience in evaluating the known benefits, risks, and limitations of a clinician’s recommendations for screening, prevention, treatment, and follow-up. As a result, shared decision-making also respects a patient’s autonomy, agency, and capacity in defining and managing their healthcare goals. Building a clinician-patient relationship rooted in shared decision-making can help clinicians engage in productive discussions with patients whose decisions may not align with optimal health outcomes. Fostering open and honest dialogue to understand a patient’s motivations while suspending judgment to reduce harm and explore alternatives is particularly vital when a patient chooses to engage in practices that may exacerbate or complicate health conditions [Halperin, et al. 2007].
Options: Implicit in the shared decision-making process is the recognition that the “right” healthcare decisions are those made by informed patients and clinicians working toward patient-centered and defined healthcare goals. When multiple options are available, shared decision-making encourages thoughtful discussion of the potential benefits and potential harms of all options, which may include doing nothing or waiting. This approach also acknowledges that efficacy may not be the most important factor in a patient’s preferences and choices [Sewell, et al. 2021].
Clinician awareness: The collaborative process of shared decision-making is enhanced by a clinician’s ability to demonstrate empathic interest in the patient, avoid stigmatizing language, employ cultural humility, recognize systemic barriers to equitable outcomes, and practice strategies of self-awareness and mitigation against implicit personal biases [Parish, et al. 2019].
Caveats: It is important for clinicians to recognize and be sensitive to the inherent power and influence they maintain throughout their interactions with patients. A clinician’s identity and community affiliations may influence their ability to navigate the shared decision-making process and develop a therapeutic alliance with the patient and may affect the treatment plan [KFF 2023; Greenwood, et al. 2020]. Furthermore, institutional policy and regional legislation, such as requirements for parental consent for gender-affirming care for transgender people or insurance coverage for sexual health care, may infringe upon a patient’s ability to access preventive- or treatment-related care [Sewell, et al. 2021].
Figure 1: Elements of Shared Decision-Making
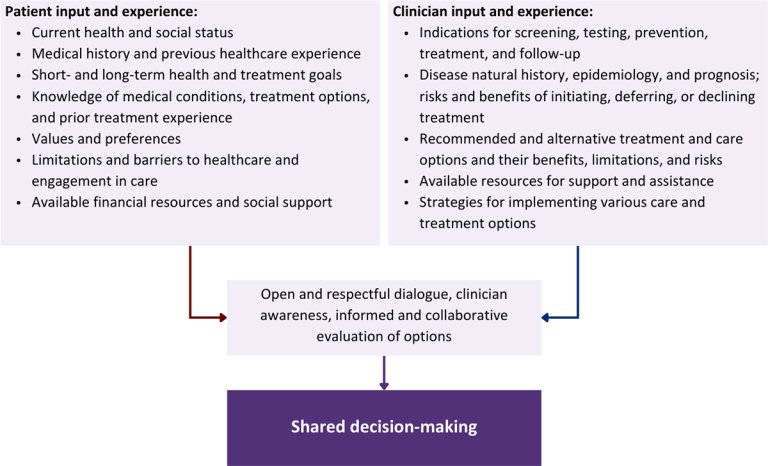
Download figure: Elements of Shared Decision-Making
Health equity: Adapting a shared decision-making approach that supports diverse populations is necessary to achieve more equitable and inclusive health outcomes [Castaneda-Guarderas, et al. 2016]. For instance, clinicians may need to incorporate cultural- and community-specific considerations into discussions with women, gender-diverse individuals, and young people concerning their sexual behaviors, fertility intentions, and pregnancy or lactation status. Shared decision-making offers an opportunity to build trust among marginalized and disenfranchised communities by validating their symptoms, values, and lived experience. Furthermore, it can allow for improved consistency in patient screening and assessment of prevention options and treatment plans, which can reduce the influence of social constructs and implicit bias [Castaneda-Guarderas, et al. 2016].
Clinician bias has been associated with health disparities and can have profoundly negative effects [FitzGerald and Hurst 2017; Hall, et al. 2015]. It is often challenging for clinicians to recognize and set aside personal biases and to address biases with peers and colleagues. Consciously or unconsciously, negative or stigmatizing assumptions are often made about patient characteristics, such as race, ethnicity, gender, sexual orientation, mental health, and substance use [Avery, et al. 2019; van Boekel, et al. 2013; Livingston, et al. 2012]. With its emphasis on eliciting patient information, a shared decision-making approach encourages clinicians to inquire about patients’ lived experiences rather than making assumptions and to recognize the influence of that experience in healthcare decision-making.
Stigma: Stigma may prevent individuals from seeking or receiving treatment and harm reduction services [Tsai, et al. 2019]. Among people with HIV, stigma and medical mistrust remain significant barriers to healthcare utilization, HIV diagnosis, and medication adherence and can affect disease outcomes [Turan, et al. 2017; Chambers, et al. 2015], and stigma among clinicians against people who use substances has been well-documented [Stone, et al. 2021; Tsai, et al. 2019; van Boekel, et al. 2013]. Sexual and reproductive health, including strategies to prevent HIV transmission, acquisition, and progression, may be subject to stigma, bias, social influence, and violence.
| SHARED DECISION-MAKING IN HIV CARE |
|
Resources and Suggested Reading
In addition to the references cited below, the following resources and suggested reading may be useful to clinicians.
| RESOURCES |
References
Acree ME, McNulty M, Blocker O, et al. Shared decision-making around anal cancer screening among black bisexual and gay men in the USA. Cult Health Sex 2020;22(2):201-16. [PMID: 30931831]
Avery JD, Taylor KE, Kast KA, et al. Attitudes toward individuals with mental illness and substance use disorders among resident physicians. Prim Care Companion CNS Disord 2019;21(1):18m02382. [PMID: 30620451]
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med 2011;24(3):229-39. [PMID: 21551394]
Castaneda-Guarderas A, Glassberg J, Grudzen CR, et al. Shared decision making with vulnerable populations in the emergency department. Acad Emerg Med 2016;23(12):1410-16. [PMID: 27860022]
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health 2015;15:848. [PMID: 26334626]
Chen CH, Kang YN, Chiu PY, et al. Effectiveness of shared decision-making intervention in patients with lumbar degenerative diseases: a randomized controlled trial. Patient Educ Couns 2021;104(10):2498-2504. [PMID: 33741234]
Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, et al. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore) 2020;99(32):e21389. [PMID: 32769870]
Coulter A, Collins A. Making shared decision-making a reality: no decision about me, without me. 2011. https://www.kingsfund.org.uk/sites/default/files/Making-shared-decision-making-a-reality-paper-Angela-Coulter-Alf-Collins-July-2011_0.pdf
Crawford J, Petrie K, Harvey SB. Shared decision-making and the implementation of treatment recommendations for depression. Patient Educ Couns 2021;104(8):2119-21. [PMID: 33563500]
FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics 2017;18(1):19. [PMID: 28249596]
Greenwood BN, Hardeman RR, Huang L, et al. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020;117(35):21194-21200. [PMID: 32817561]
Groot G, Waldron T, Barreno L, et al. Trust and world view in shared decision making with indigenous patients: a realist synthesis. J Eval Clin Pract 2020;26(2):503-14. [PMID: 31750600]
Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health 2015;105(12):e60-76. [PMID: 26469668]
Halperin B, Melnychuk R, Downie J, et al. When is it permissible to dismiss a family who refuses vaccines? Legal, ethical and public health perspectives. Paediatr Child Health 2007;12(10):843-45. [PMID: 19043497]
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. 2001. https://www.ncbi.nlm.nih.gov/books/NBK222274/
KFF. Key data on health and health care by race and ethnicity. 2023 Mar 15. https://www.kff.org/racial-equity-and-health-policy/report/key-data-on-health-and-health-care-by-race-and-ethnicity/ [accessed 2023 May 19]
Livingston JD, Milne T, Fang ML, et al. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction 2012;107(1):39-50. [PMID: 21815959]
McNulty MC, Acree ME, Kerman J, et al. Shared decision making for HIV pre-exposure prophylaxis (PrEP) with black transgender women. Cult Health Sex 2022;24(8):1033-46. [PMID: 33983866]
Niburski K, Guadagno E, Abbasgholizadeh-Rahimi S, et al. Shared decision making in surgery: a meta-analysis of existing literature. Patient 2020;13(6):667-81. [PMID: 32880820]
Parish SJ, Hahn SR, Goldstein SW, et al. The International Society for the Study of Women’s Sexual Health process of care for the identification of sexual concerns and problems in women. Mayo Clin Proc 2019;94(5):842-56. [PMID: 30954288]
Robinson JH, Callister LC, Berry JA, et al. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008;20(12):600-607. [PMID: 19120591]
Scalia P, Durand MA, Elwyn G. Shared decision-making interventions: an overview and a meta-analysis of their impact on vaccine uptake. J Intern Med 2022;291(4):408-25. [PMID: 34700363]
Sewell WC, Solleveld P, Seidman D, et al. Patient-led decision-making for HIV preexposure prophylaxis. Curr HIV/AIDS Rep 2021;18(1):48-56. [PMID: 33417201]
Stalnikowicz R, Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract 2020;26(2):431-38. [PMID: 31989727]
Stone EM, Kennedy-Hendricks A, Barry CL, et al. The role of stigma in U.S. primary care physicians’ treatment of opioid use disorder. Drug Alcohol Depend 2021;221:108627. [PMID: 33621805]
Tsai AC, Kiang MV, Barnett ML, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med 2019;16(11):e1002969. [PMID: 31770387]
Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav 2017;21(1):283-91. [PMID: 27272742]
van Boekel LC, Brouwers EP, van Weeghel J, et al. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013;131(1-2):23-35. [PMID: 23490450]
References
Carveth-Johnson T., Stingone C., Nwokolo N., et al. Doxycycline use in MSM taking PrEP. Lancet HIV 2018;5(9):e482. [PMID: 30215346]
CDC. Sexually transmitted disease surveillance 2021. 2023 Apr 11. https://www.cdc.gov/std/statistics/2021/default.htm [accessed 2023 Apr 24]
CDPH. Doxycycline post-exposure prophylaxis (doxy-PEP) for the prevention of bacterial sexually transmitted infections (STIs). 2023 Apr 28. https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/CDPH-Doxy-PEP-Recommendations-for-Prevention-of-STIs.pdf [accessed 2023 June 12]
Chow E. P. F., Fairley C. K. Use of doxycycline prophylaxis among gay and bisexual men in Melbourne. Lancet HIV 2019;6(9):e568-69. [PMID: 31498105]
Cornelisse V. J., Ong J. J., Ryder N., et al. Interim position statement on doxycycline post-exposure prophylaxis (doxy-PEP) for the prevention of bacterial sexually transmissible infections in Australia and Aotearoa New Zealand - the Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM). Sex Health 2023;20(2):99-104. [PMID: 36927481]
Evers Y. J., van Liere G., Dukers-Muijrers N., et al. Use of doxycycline and other antibiotics to prevent STIs among men who have sex with men visiting sexual health clinics in the Netherlands. Sex Transm Infect 2020;96(7):550-51. [PMID: 31879360]
Fairley C. K., Chow E. P. Doxycycline post-exposure prophylaxis: let the debate begin. Lancet Infect Dis 2018;18(3):233-34. [PMID: 29229439]
FDA. Doxycycline hyclate delayed-release tablets, for oral use. 2016 Apr. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/90431Orig1s010lbl.pdf [accessed 2023 June 12]
Fusca L., Hull M., Ross P., et al. High interest in syphilis pre-exposure and post-exposure prophylaxis among gay, bisexual and other men who have sex with men in Vancouver and Toronto. Sex Transm Dis 2020;47(4):224-31. [PMID: 31977974]
Gandhi R. T., Bedimo R., Hoy J. F., et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2022 recommendations of the International Antiviral Society-USA Panel. JAMA 2023;329(1):63-84. [PMID: 36454551]
Golden M. R., Handsfield H. H. Preexposure prophylaxis to prevent bacterial sexually transmitted infections in men who have sex with men. Sex Transm Dis 2015;42(2):104-6. [PMID: 25585070]
Grant J. S., Stafylis C., Celum C., et al. Doxycycline prophylaxis for bacterial sexually transmitted infections. Clin Infect Dis 2020;70(6):1247-53. [PMID: 31504345]
Haaland R., Fountain J., Dinh C., et al. Mucosal pharmacology of doxycycline for bacterial STI prevention in men and women. Abstract 118. CROI; 2023 Feb 19-22; Seattle, WA. https://www.croiconference.org/abstract/mucosal-pharmacology-of-doxycycline-for-bacterial-sti-prevention-in-men-and-women/
Kohli M., Medland N., Fifer H., et al. BASHH updated position statement on doxycycline as prophylaxis for sexually transmitted infections. Sex Transm Infect 2022;98(3):235-36. [PMID: 35414633]
Lewis D. Push to use antibiotics to prevent sexually transmitted infections raises concerns. Nature 2022;612(7938):20-21. [PMID: 36418876]
Lexicomp. Doxycycline (Lexi-Drugs). 2023 Sep 16. https://online.lexi.com/lco/action/doc/retrieve/docid/patch_f/6792?searchUrl=%2Flco%2Faction%2Fsearch%3Forigin%3Dapi%26t%3Dglobalid%26q%3D6077%26nq%3Dtrue [accessed 2023 Jun 12]
Luetkemeyer A. F., Dombrowski J. C., Cohen S., et al. Doxycycline post-exposure prophylaxis for STI prevention among MSM and transgender women on HIV PrEP or living with HIV: high efficacy to reduce incident STIs in a randomized trial. AIDS; 2022 July 29 - Aug 2; Montreal, Canada. https://programme.aids2022.org/Abstract/Abstract/?abstractid=13231
Luetkemeyer A. F., Donnell D., Dombrowski J. C., et al. Postexposure doxycycline to prevent bacterial sexually transmitted infections. N Engl J Med 2023;388(14):1296-1306. [PMID: 37018493]
Molina J. M., Bercot B., Assoumou L., et al. ANRS 174 DOXYVAC: an open-label randomized trial to prevent STIs in MSM on PrEP. Abstract 119. CROI; 2023 Feb 19-22; Seattle, WA. https://www.croiconference.org/abstract/anrs-174-doxyvac-an-open-label-randomized-trial-to-prevent-stis-in-msm-on-prep/
Molina J. M., Charreau I., Chidiac C., et al. Post-exposure prophylaxis with doxycycline to prevent sexually transmitted infections in men who have sex with men: an open-label randomised substudy of the ANRS IPERGAY trial. Lancet Infect Dis 2018;18(3):308-17. [PMID: 29229440]
NCSD. Doxycycline for STI PEP implementation toolkit. 2023 Jul. https://www.ncsddc.org/wp-content/uploads/2023/07/Doxycycline-as-STI-PEP-Toolkit-July-2023.pdf [accessed 2023 Aug 3]
O'Halloran C., Croxford S., Mohammed H., et al. Factors associated with reporting antibiotic use as STI prophylaxis among HIV PrEP users: findings from a cross-sectional online community survey, May-July 2019, UK. Sex Transm Infect 2021;97(6):429-33. [PMID: 33082235]
Osmon D. R., Berbari E. F., Berendt A. R., et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2013;56(1):e1-25. [PMID: 23223583]
Park J. J., Stafylis C., Pearce D. D., et al. Interest, concerns, and attitudes among men who have sex with men and health care providers toward prophylactic use of doxycycline against Chlamydia trachomatis infections and syphilis. Sex Transm Dis 2021;48(9):615-19. [PMID: 33560092]
PHSKC. Doxycycline post-exposure prophylaxis (doxy-PEP) to prevent bacterial STIs in men who have sex with men (MSM) and transgender persons who have sex with men. 2023 Mar 20. https://kingcounty.gov/depts/health/communicable-diseases/~/media/depts/health/communicable-diseases/documents/hivstd/DoxyPEP-Guidelines.ashx [accessed 2023 Aug 3]
SCPHD. Doxycycline use as post-exposure prophylaxis to prevent bacterial sexually transmitted infections. 2023 Mar 20. https://publichealthproviders.sccgov.org/sites/g/files/exjcpb951/files/documents/doxypep_guidance.pdf [accessed 2023 Aug 3]
SFDPH. Health update: doxycycline post-exposure prophylaxis reduces incidence of sexually transmitted infections. 2022 Oct 20. https://www.sfcdcp.org/wp-content/uploads/2022/10/Health-Update-Doxycycline-Post-Exposure-Prophylaxis-Reduces-Incidence-of-Sexually-Transmitted-Infections-SFDPH-FINAL-10.20.2022.pdf [accessed 2023 Apr 24]
Siguier M., Molina J. M. Doxycycline prophylaxis for bacterial sexually transmitted infections: promises and perils. ACS Infect Dis 2018;4(5):660-63. [PMID: 29570279]
Soge O. O., Issema R., Bukusi E., et al. Predominance of high-level tetracycline-resistant Neisseria gonorrhoeae in Kenya: implications for global implementation of doxycycline post-exposure prophylaxis for prevention of sexually transmitted infections. Sex Transm Dis 2023;50(5):317-19. [PMID: 36728331]
Spinelli M. A., Scott H. M., Vittinghoff E., et al. High interest in doxycycline for sexually transmitted infection postexposure prophylaxis in a multicity survey of men who have sex with men using a social networking application. Sex Transm Dis 2019;46(4):e32-34. [PMID: 30870327]
Stewart J., Oware K., Donell D., et al. Doxycycline postexposure prophylaxis for prevention of STIs among cisgender women. Abstract 121. CROI; 2023 Feb 19-22; Seattle, WA. https://www.croiconference.org/abstract/doxycycline-postexposure-prophylaxis-for-prevention-of-stis-among-cisgender-women/
Traeger M. W., Mayer K. H., Krakower D. S., et al. Potential impact of doxycycline post-exposure prophylaxis prescribing strategies on incidence of bacterial sexually transmitted infections. Clin Infect Dis 2023. [PMID: 37595139]
Vanbaelen T., Manoharan-Basil S. S., Kenyon C. Doxycycline postexposure prophylaxis could induce cross-resistance to other classes of antimicrobials in Neisseria gonorrhoeae: an in silico analysis. Sex Transm Dis 2023;50(8):490-93. [PMID: 36952471]
Wilson D. P., Prestage G. P., Gray R. T., et al. Chemoprophylaxis is likely to be acceptable and could mitigate syphilis epidemics among populations of gay men. Sex Transm Dis 2011;38(7):573-79. [PMID: 21343845]
Workowski K. A., Bachmann L. H., Chan P. A., et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep 2021;70(4):1-187. [PMID: 34292926]
Zaenglein A. L., Pathy A. L., Schlosser B. J., et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol 2016;74(5):945-73.e33. [PMID: 26897386]
Updates, Authorship, and Related Guidelines
| Updates, Authorship, and Related Guidelines | |
| Date of original publication | September 25, 2023 |
| Intended users | New York State clinicians who provide medical care for individuals at risk of acquiring sexually transmitted infections |
| Lead author(s) |
Daniela E. DiMarco, MD, MPH; Marguerite A. Urban, MD |
| Writing group |
Steven M. Fine, MD; Rona M. Vail, MD; Joseph P. McGowan, MD, FACP, FIDSA; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Jessica Rodrigues, MS; Charles J. Gonzalez, MD; Christopher J. Hoffmann, MD, MPH |
| Author and writing group conflict of interest disclosures | There are no author or writing group conflict of interest disclosures. |
| Committee | |
| Developer and funder |
New York State Department of Health AIDS Institute (NYSDOH AI) |
| Development process |
See Guideline Development and Recommendation Ratings Scheme, below. |
| Related NYSDOH AI guidelines | |
Guideline Development and Recommendation Ratings
| Guideline Development: New York State Department of Health AIDS Institute Clinical Guidelines Program | |
| Program manager | Clinical Guidelines Program, Johns Hopkins University School of Medicine, Division of Infectious Diseases. See Program Leadership and Staff. |
| Mission | To produce and disseminate evidence-based, state-of-the-art clinical practice guidelines that establish uniform standards of care for practitioners who provide prevention or treatment of HIV, viral hepatitis, other sexually transmitted infections, and substance use disorders for adults throughout New York State in the wide array of settings in which those services are delivered. |
| Expert committees | The NYSDOH AI Medical Director invites and appoints committees of clinical and public health experts from throughout New York State to ensure that the guidelines are practical, immediately applicable, and meet the needs of care providers and stakeholders in all major regions of New York State, all relevant clinical practice settings, key New York State agencies, and community service organizations. |
| Committee structure |
|
| Disclosure and management of conflicts of interest |
|
| Evidence collection and review |
|
| Recommendation development |
|
| Review and approval process |
|
| External reviews |
|
| Update process |
|
| Recommendation Ratings Scheme | |||
| Strength | Quality of Evidence | ||
| Rating | Definition | Rating | Definition |
| A | Strong | 1 | Based on published results of at least 1 randomized clinical trial with clinical outcomes or validated laboratory endpoints. |
| B | Moderate | * | Based on either a self-evident conclusion; conclusive, published, in vitro data; or well-established practice that cannot be tested because ethics would preclude a clinical trial. |
| C | Optional | 2 | Based on published results of at least 1 well-designed, nonrandomized clinical trial or observational cohort study with long-term clinical outcomes. |
| 2† | Extrapolated from published results of well-designed studies (including nonrandomized clinical trials) conducted in populations other than those specifically addressed by a recommendation. The source(s) of the extrapolated evidence and the rationale for the extrapolation are provided in the guideline text. One example would be results of studies conducted predominantly in a subpopulation (e.g., one gender) that the committee determines to be generalizable to the population under consideration in the guideline. | ||
| 3 | Based on committee expert opinion, with rationale provided in the guideline text. | ||
Last updated on March 6, 2024