
Purpose of This Guideline
Date of current publication: February 10, 2026
Lead author: Joseph P. McGowan, MD, FACP, FIDSA, AAHIVS
Writing group: Rona M. Vail, MD, AAHIVS; Sanjiv S. Shah, MD, MPH, AAHIVS; Steven M. Fine, MD, PhD; Samuel T. Merrick, MD, FIDSA; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Jessica Rodrigues, MPH, MS; Christopher J. Hoffmann, MD, MPH, MSc, FACP; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: November 29, 2022
Purpose: This guideline was developed by the New York State Department of Health AIDS Institute (NYSDOH AI) Medical Care Criteria Committee to provide New York State clinicians with effective care management strategies for patients with HIV who require changes in their antiretroviral therapy (ART) regimens. Effective ART has allowed individuals with HIV to live longer and healthier lives than patients diagnosed earlier in the epidemic. Modern ART options are effective, safe, and simple, and guidance on their use for treatment-naive patients is available in the NYSDOH AI guideline Selecting an Initial ART Regimen and DHHS Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents With HIV. However, clinical scenarios may arise in which a patient’s ART is ineffective, leading to virologic failure, adverse effects, or drug-drug interactions with other essential medications; older ART regimens may also be burdensome for patients who may benefit from simplification.
Goals: This guideline provides information to assist clinicians in making evidence-based decisions to change ART regimens and formulate second-line and subsequent ART regimens for optimal viral suppression in patients with HIV. Toward that end, the goals of this guideline are to:
- Increase clinicians’ ability to recognize ART failure
- Increase clinicians’ ability to effectively manage switching a patient’s initial or subsequent ART regimen when indicated to:
- Improve viral suppression
- Recognize and respond to virologic failure in a timely fashion
- Improve tolerability
- Reduce toxic effects
- Avoid drug-drug interactions
- Simplify (i.e., change from a multi-tablet regimen to a single-tablet regimen)
- Ensure safety during pregnancy
- Assist clinicians in managing a patient’s resumption of ART after a treatment interruption
- Assist clinicians in recognizing cases that may benefit from expert consultation, such as when choosing a new ART regimen for a patient who has already been treated with multiple ART regimens or has other complicating factors
- Encourage clinicians to seek the assistance of an experienced HIV care provider when treating patients with extensive resistance to antiretroviral drugs
Defining treatment failure: This guideline focuses on strategies for changing ART regimens to address 2 types of ART treatment failure—virologic failure and failure due to adverse effects or intolerance. The guideline also addresses modifications of suppressive therapy to avoid drug interactions with concomitant medications or to simplify ART to enhance tolerability and adherence (for more information, see guideline section Identifying and Managing Virologic Failure > Defining Virologic Failure).
This guideline does not focus on immunologic failure, sometimes referred to as a “CD4/viral load disconnect,” which is defined as a fully suppressed HIV viral load on ART without a restoration of CD4 count above a target threshold, such as 200 or 500 cells/mm3. Immunologic failure has been associated with increased age and low CD4 cell count (nadir) at treatment initiation Prabhakar, et al. 2011. Studies have indicated that excess morbidity and mortality can occur if the CD4 count remains below 500 cells/mm3 Lewden, et al. 2012. No specific interventions or use of immune-based therapy, such as interleukin-2, have persistently improved CD4 counts, and immune-based therapy may increase immune activation, which can be detrimental to viral reservoir control Abrams, et al. 2009. It is appropriate to treat active infections, including opportunistic infections, but incomplete CD4 recovery may persist if ongoing immune activation is present Lederman, et al. 2011. Switching ART for a patient with viral suppression would not significantly affect CD4 recovery or decrease immune activation Hunt, et al. 2013.
Note on “experienced” HIV care providers: The NYSDOH AI Clinical Guidelines Program defines an “experienced HIV care provider” as a practitioner who has been accorded HIV Specialist status by the American Academy of HIV Medicine. Nurse practitioners (NPs) and licensed midwives who provide clinical care to individuals with HIV in collaboration with a physician may be considered experienced HIV care providers if all other practice agreements are met; NPs with more than 3,600 hours of qualifying experience do not require collaboration with a physician (8 NYCRR 79-5:1; 10 NYCRR 85.36; 8 NYCRR 139-6900). Physician assistants who provide clinical care to individuals with HIV under the supervision of an HIV Specialist physician may also be considered experienced HIV care providers (10 NYCRR 94.2).
Identifying and Managing Virologic Failure
| RECOMMENDATIONS |
Identifying and Managing Virologic Failure
|
Defining Virologic Failure
Virologic failure is defined as a confirmed HIV viral load ≥200 copies/mL despite a patient’s use of recommended ART for at least 24 weeks or a viral load that rebounds to ≥200 copies/mL after a patient achieves viral suppression. When unsuppressed, persistent HIV replication leads to the development of resistance-associated mutations (RAMs), loss of CD4 T-helper cells, and associated clinical consequences. Table 1, below, summarizes types of HIV resistance tests and their uses.
RAMs represent alterations of HIV genetic code at specific locations, such as the gene that encodes the reverse transcriptase enzyme that copies the viral RNA into DNA, the protease gene that processes viral proteins, or the integrase gene that enables viral genes to be incorporated into host chromosomal DNA. These alterations lead to a substitution (change) in the usual amino acid pattern of that protein that has been linked to decreased activity of a drug used to block it. For example, the most common RAM is the M184V mutation of the reverse transcriptase gene selected by use of emtricitabine or lamivudine, in which the amino acid valine at position 184 of the encoding gene is substituted for the usual methionine Shafer and Schapiro 2008. The mutation allows the enzyme to function and the virus to replicate in the presence of the drug. Mutations that do not lead to amino acid changes or that do not affect the function of antiretroviral medications (ARVs) would be silent and not be counted as RAMs.
| Abbreviations: ART, antiretroviral therapy; ARV, antiretroviral medication; gp120, envelope glycoprotein 120; RAM, resistance-associated mutation.
Note:
|
||
| Table 1: Types of HIV Resistance Tests [a] | ||
| Test | Description | Use |
| Genotype |
|
|
| Phenotype |
|
|
| Proviral DNA genotype (archived DNA genotype) |
|
|
| Tropism test | Assesses the effect of HIV RNA (or proviral DNA) gp120 on the coreceptor(s) used for viral attachment: CCR5, CXCR4, or mixed/dual |
|
Persistent low-level viremia: Persistent, even low-level, HIV viremia quantifiable above the lower limit of assay detection for at least 1 month is associated with increased all-cause mortality, AIDS events, and development of RAMs Elvstam, et al. 2021; Bernal, et al. 2018; Elvstam, et al. 2017; Vandenhende, et al. 2015; Ryscavage, et al. 2014; Delaugerre, et al. 2012. At low levels of viremia, the error-prone HIV reverse transcriptase creates RAMs under the selective pressure of ART, causing ART to lose efficacy. Persistent low-level viremia has been found more often in treatment-experienced patients than in those on initial ART, suggesting that unrecognized preexisting resistance may contribute to treatment failure Ferretti, et al. 2019; Fleming, et al. 2019. Persistent low-level viremia (≥2 consecutive HIV viral load measures between 50 and 199 copies/mL) remains an important marker of risk for treatment failure even with use of highly potent ARVs with a high genetic barrier to resistance. In a cohort study of 451 participants with HIV who had low-level viremia, virologic suppression was significantly higher for those who switched their ART regimen, including 296 participants who were taking a regimen with a high genetic barrier to resistance at baseline Clemente, et al. 2025.
Low-level viremia has been specifically associated with protease inhibitor (PI)-based treatment. One explanation for this finding may be prescriber bias in choosing PIs if adherence is a concern. Another explanation could be that when viral reservoirs are high (high pretreatment viral loads or prolonged unsuppressed viremia), the immature virions released on PI therapy are measurable Sedaghat, et al. 2008. A third possibility is that low-level viremia could result from mutations developing in the gag polyprotein gene at the protease cleavage sites, which would not be reported on standard population genotyping Fleming, et al. 2019.
However, not all causes of low-level viremia have the same implications. Low-level viremia in patients with poor or intermittent adherence increases the risk of treatment failure, whereas the same level of viremia with consistent adherence in the absence of underlying resistance does not. Therefore, adherence is the first issue to address when low-level viremia is detected, and a change in ART is required to address any identified preexisting mutations (see discussion of proviral DNA genotyping in Resistance-Associated Mutations, below). One retrospective study of patients taking ART who had residual detected viremia (viral load 50 to 500 copies/mL) found a reduction of viral load following intensification with the CCR5 antagonist maraviroc [Dû, et al. 2016]. The underlying cause of persistent low-level viremia may be difficult to discern clinically. Therefore, instead of intensifying by adding a single agent, it is advisable to assess or, if needed, modify an existing regimen to optimize use of active agents, such as by including drugs with high barriers to resistance Crespo-Bermejo, et al. 2021.
If adherence is not a problem and no RAMs have been identified, low-level detectable virus (viral load <200 copies/mL) may be a reflection of the viral reservoir size or the consequence of proviral DNA integration into an active, constitutively replicating gene in the CD4 chromosome that produces virus ongoing from a single infected clone Mohammadi, et al. 2023; Halvas, et al. 2020; Jacobs, et al. 2019. In these circumstances, treatment intensification would not reduce a detectable viral load and a switch to treatment with a nucleoside/nucleotide reverse transcriptase inhibitor (NRTI) plus a PI could inactivate the post-transcriptional virus and prevent the next cycle of reverse transcription, which may be an important consideration in individuals at risk for HIV transmission. The likelihood that clonal-derived viremia will persist beyond 48 weeks appears relative to the proportion of viral load measures with ≥40 copies/mL Halvas, et al. 2024.
The source of persistent very low-level viremia (viral load <50 copies/mL) has been debated Ryscavage, et al. 2014. It may emerge from ongoing viral replication, which is prone to reverse-transcriptase-induced development of RAMs, or it could be the result of post-integration release from the viral reservoir (clonal origin); clonal origin virus is blocked from infecting new cells by the presence of ongoing active ART. Intensifying treatment by adding a new non-nucleoside reverse transcriptase inhibitor (NNRTI), PI, CCR5 antagonist, or integrase strand transfer inhibitor (INSTI) to an ART regimen has not been shown to reduce residual viral load or immune activation in patients with a viral load <50 copies/mL Gutiérrez, et al. 2011; Gandhi, et al. 2010; Dinoso, et al. 2009.
Studies evaluating the evolution of viral genetic mutations in proviral DNA following infection have indicated an arrest of widening diversity after the introduction of suppressive ART Kearney, et al. 2014. These findings demonstrate that residual viremia likely emerges from preestablished viral reservoirs through stimulation of post-integration virus rather than through replication via mutation-prone reverse transcription and would not be suppressed by adding ARVs to existing ART regimens. This is supported by several studies demonstrating that treatment intensification, such as adding an INSTI to an existing ART regimen, does not affect the viral load Gandhi, et al. 2010; McMahon, et al. 2010; Steigbigel, et al. 2008. Although ART modification does not decrease viremia if replication is fully suppressed, it is often clinically challenging to assess the effect of complicating factors, such as adherence and drug or food interactions, on measured low-level viremia; therefore, some experts would use only an ART regimen that contains an agent with a high genetic barrier to resistance in such situations.
Blips: Occasionally, the detection of low-level viremia is an isolated event, and viral suppression is confirmed on a repeat viral load test. These events are called “blips” if they are in the range of 20 to 200 copies/mL and are preceded and followed by viral load measurements of <20 copies/mL (i.e., full viral suppression). Blips have not been found to increase future risk of virologic failure Havlir, et al. 2001. The increased sensitivity of HIV viral load assays allows the detection of viral load levels as low as 20 copies/mL. Transient low-level viremia may also be the result of T-cell activation associated with acute infections, opportunistic infections, post-vaccination blips, and chronic immune activation, which should be considered when clinically indicated, such as during immune reconstitution following ART initiation to diagnosed or unmasked infections Matveev, et al. 2023; Raccagni, et al. 2023; Younas, et al. 2021; Jones and Perelson 2005. Quantifiable HIV viremia <50 copies/mL has not been associated with subsequent therapeutic failure or emergence of drug resistance Teira, et al. 2017. In cases of very low-level viremia or blips, adjustment of the ART regimen is not required.
| KEY POINTS |
|
Causes of Virologic Failure
Virologic failure may occur for several reasons, and a timely investigation is imperative to prevent RAMs and subsequent loss of immune function. The most likely causes of ART-associated virologic failure are poor adherence, pharmacokinetic drug-drug interactions that lead to subtherapeutic target drug concentrations, and the presence (through transmission) or development of drug resistance mutations. The time it takes for drug resistance to emerge is related to several factors, including the height of the residual viral load, the level of drug exposure, the specific medications used, and the patient’s pattern of adherence. Virologic failure can occur within months or within weeks, especially because a single RAM can lead to failure for some medications Feder(b), et al. 2021.
Adherence: Poor or incomplete adherence, commonly defined as less than 90% to 95% of doses taken, is one of the most common reasons for virologic failure or relapse Ortego, et al. 2011. It is important to verify that the patient can identify their ART medications and confirm pharmacy refills to ensure proper access as part of an adherence assessment. Poor ART adherence has been associated with younger age, male sex, Black race, low income and education level, injection drug use, alcohol use, and lack of effective adherence support Papageorgiou, et al. 2022; Benson, et al. 2020. Patients who experience adverse effects may not adhere to their ART regimen or may stop taking the medications altogether. Other barriers to adherence include inability to pay for medications, substance use, housing instability, health literacy, language barriers, concerns about drug-drug interactions (e.g., between gender-affirming hormone therapy and ART) Braun, et al. 2017, and mental illness. Identifying and addressing modifiable barriers and providing support for optimal adherence are crucial. Socioeconomic barriers, internalized HIV stigma, financial limitations, unstable housing, and disbelief in treatment value may also reduce adherence. Young adults and adolescents are at particularly high risk of poor ART adherence Kim, et al. 2014. Routine patient education and a multidisciplinary approach are key to addressing these issues. Inclusion of peers to facilitate adherence to ART regimens is effective, and peers are viewed as credible sources for health information Enriquez, et al. 2019; Houston, et al. 2015.
Forgetfulness is a modifiable factor that can be addressed by dispensing ART medications in prefilled pill trays or dose packs, monitoring pharmacy refill patterns; setting up digital alerts; sending messages from healthcare providers, peers, or case managers; encouraging support from family or friends; linking medication timing to routine daily activities; or using long-acting injectable medications. Management of chronic comorbidities and coinfections often adds a significant number of daily medications, which may complicate a patient’s ability to adhere to an ART regimen. ART simplification to lower pill burden is addressed in the guideline section ART Changes for Regimen Simplification.
Identifying and addressing the adherence problems causing virologic failure can prevent unnecessary ART intensification. Treatment intensification can further complicate adherence and expose additional classes of ARVs to the risk of resistance development. If virologic failure is detected in a patient taking a complete ART regimen who does not report missing doses, genotypic resistance testing should be performed. A standard genotype test is appropriate if the patient’s HIV viral load is ≥500 copies/mL Swenson, et al. 2014; an archive genotype test may be considered if a persistently detectable viral load below that level is found.
The hallmark of nonadherence as the cause of virologic failure is the presence of wild-type virus (i.e., no pertinent RAMs) or a genotype test result indicating that the prevalent viral population is fully susceptible to the prescribed ART regimen. Susceptible virus should be suppressed; resistant virus predominates in the presence of full selective pressure. In these cases, it is essential to identify and address adherence challenges. It may be appropriate to select a single-tablet regimen with higher forgiveness for incomplete adherence (or higher “genetic barrier”), such as a boosted PI or second-generation INSTI-based regimen Anstett, et al. 2017. The preferred agents from these classes in the absence of baseline resistance are:
- Tenofovir alafenamide/emtricitabine/bictegravir (TAF 25 mg/FTC/BIC; Biktarvy); or
- Tenofovir alafenamide/emtricitabine/cobicistat/darunavir (TAF 10 mg/FTC/COBI/ DRV; Symtuza).
Resistance-Associated Mutations
“Transmitted resistance” refers to RAMs present at the time of HIV acquisition (see Table 2, below, for prevalence of transmitted RAMs). To construct a fully suppressive ART regimen, clinicians have to first recognize these mutations, which requires baseline genotypic resistance testing before ART initiation to identify any highly represented strains. Regimens recommended for same-day or rapid ART initiation have been selected for activity against virus containing the most prevalent transmitted RAMs.
| Abbreviations: INSTI, integrase strand transfer inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside/nucleotide reverse transcriptase inhibitor; PI, protease inhibitor; RAM, resistance-associated mutation. | |
| Table 2: Prevalence of Transmitted HIV Drug Resistance-Associated Mutations | |
| Population | Prevalence of RAMs |
| 36,288 genotype sequences from individuals who acquired HIV in the United States between 2013 and 2016 McClung, et al. 2022 |
Transmitted: 19.0%
|
| 3,616 genotype sequences acquired from ART-naive individuals in California from 2008 to 2018 Feng, et al. 2020 |
Transmitted: 20.0%
|
Multiclass drug resistance: The emergence of multiclass drug-resistant virus presents challenges in managing ART. Rates of “triple class” (NRTI, NNRTI, and PI) resistance were found in 10% of longitudinal care patients at a U.S. HIV specialty center, where multiclass drug resistance was associated with low CD4 count and high viral load at ART initiation, prolonged ART use, initiation with non-highly active ART regimens, or use of many different ARVs over many years Davy-Mendez, et al. 2018; Napravnik, et al. 2007. In the multicenter Pediatric HIV/AIDS Cohort Study, the rate of triple-class-resistant virus was 18% among individuals with perinatally acquired HIV Van Dyke, et al. 2016.
With the advent of INSTIs, attachment inhibitors, and capsid inhibitors, many individuals with triple-class-resistant virus can now achieve viral suppression. Treatment failure with first-generation INSTIs (raltegravir or elvitegravir) has been associated with significant cross-resistance to the second-generation INSTIs dolutegravir and bictegravir Orta-Resendiz, et al. 2020. As ART regimens have been simplified, it appears that rates of resistance to NRTIs, NNRTIs, and PIs peaked around 2005 and may be on the decline while rates of INSTI resistance have been increasing over time Davy-Mendez, et al. 2018, to the extent that 5-class resistant viruses have now been reported Puertas, et al. 2020; Magambo, et al. 2014.
Genotypic resistance testing: Genotypic resistance testing should be performed in all cases of virologic failure Weinstein, et al. 2001. If a patient’s plasma HIV-1 viral load is ≥500 copies/mL, a standard plasma RNA genotype should be obtained; if the breakthrough viral load is <500 copies/mL, a proviral DNA genotype (archived DNA genotype) test should be obtained if viral suppression is not achieved after addressing adherence and drug-drug interaction issues. Plasma RNA genotype testing could be attempted with viral loads <500 copies/mL; however, as the viral load decreases, the amplification success rate decreases and the likelihood of missing mutations increases due to sampling limitations.
The timing of genotyping with HIV RNA is important. A viral load ≥500 copies/mL is typically necessary to detect RAMs. A lower level of viremia may lead to assay failure. Ideally, the test should be performed while the patient is taking a failing regimen. Stopping ART would remove selective pressure and allow wild-type (nonmutated) HIV to repopulate and dilute out the resistant HIV strain, hindering the chance to identify RAMs that may have developed. If ART is stopped, resistance testing should be performed within 4 weeks. Beyond week 4, the ability to detect mutations may decay at a variable rate (transmitted mutations and those that have less effect on viral growth fitness may persist longer), making standard genotyping less reliable, in which case HIV DNA testing may be more informative Ellis, et al. 2020; Iarikov, et al. 2010.
Even with appropriate timing, both RNA and DNA genotype assays may not provide complete information because resistant strains may only be represented as a minority species and evade amplification. Therefore, it is crucial to review prior testing results for RAMs (genotypes) and phenotypic resistance test results and inquire about prior nonsuppressive ART regimens to identify likely resistance and cross-resistance patterns. Factors that increase the likelihood of virologic failure and potential RAM development include virologic breakthrough on an ART regimen with a low genetic barrier, longer time with unsuppressed viremia, treatment with an incomplete ART regimen, or partial adherence to ART Cohen, et al. 2013; Daar, et al. 2011; Riddler, et al. 2008.
RAMs can be detected by sequencing circulating plasma HIV RNA or by sequencing proviral DNA in CD4 cells (archive genotype test). RAMs appear earlier in the plasma (an average of >400 days for PI mutations) but are maintained for a longer period in the peripheral blood mononuclear cell proviral DNA archive after treatment interruption Bi, et al. 2003. The likelihood of amplifying DNA from integrated provirus is relative to its representation in the archived DNA population, which correlates with the viral load and length of the viremic period, time for viral decay, and degree of viral suppression Chu, et al. 2022. Proviral DNA genotype testing may not amplify all previously existing archived resistant HIV variants, especially after long-term viral suppression when the density of residually infected CD4 cells may be sparse (i.e., sampling effect) Derache, et al. 2015, and it may identify mutations associated with replication-defective proviral DNA Li, et al. 2021. More than 90% of proviral DNA is defective and unlikely to be replication competent because of errors and deletions that occur during replication and host-mediated antiviral effects of APOBEC3-induced hypermutation Bruner, et al. 2016. Commercially available proviral DNA assays should have interpretive algorithms that account for the presence of APOBEC mutational signatures (e.g., GenoSure Archive® HIV-1 next-generation DNA sequencing assay) Curanovic, et al. 2023. Excluding agents based on finding RAMs in proviral DNA sequencing may limit potentially active options when choosing switch regimens, as was illustrated by the CARES study, in which participants were randomized to switch from suppressive oral to long-acting injectable cabotegravir and rilpivirine (CAB/RPV LA) therapy Kityo, et al. 2024. Only 1 of the 10 participants with RPV RAMs and 1 of the 15 with CAB RAMs on baseline proviral DNA sequencing had confirmed virologic failure after switching to long-acting therapy. However, the rate of confirmed virologic failure was higher among participants with RPV RAMs (10%) or CAB RAMs (7%) on proviral DNA sequencing than those without, who had no confirmed virologic failures. The reduced effect of preexisting RPV resistance on treatment failure in this trial is at odds with prior studies of CAB/RPV LA treatment, in which preexisting RPV resistance was a major risk factor for treatment failure, and may be related to relative responses in non-B HIV subtypes Orkin, et al. 2023; Cutrell, et al. 2021. RAMs from minor variants predictive of virologic failure of the prescribed regimen may be identified on DNA sequencing in fully virally suppressed individuals Inzaule, et al. 2018, which may be related to several factors including their presence on defective provirus or across more than 1 variant selected sequentially in the population rather than all on a single virus. The proportion of archived minor variants in the population that might affect viral suppression is unknown. Guidance on the clinical use of HIV DNA genotype testing do support its use, with the above caveats, in the context of planning an ART regimen when information from past resistance testing is not available or is incomplete or when RNA assays fail to amplify (especially if planning to simplify treatment to a low genetic barrier regimen), beyond 4 weeks after treatment interruption, and when the viral load on failing treatment is too low to be amplified by RNA genotype testing Wensing, et al. 2025; Andre-Garnier, et al. 2024. Clinicians may consider consulting with an expert in managing HIV drug resistance to assist in interpreting proviral DNA genotype results.
Currently, no genotypic tropism assay is available commercially, although algorithms to predict viral tropism from genotypic sequences are under investigation. For patients with a plasma viral load ≥500 copies/mL and for whom use of a coreceptor antagonist is being imminently considered, phenotypic testing (Trofile) can be used to assess RNA tropism; in patients with lower or undetectable plasma viral loads, a DNA tropism assay (Trofile DNA) may be used.
Signature HIV capsid mutations for resistance of the capsid inhibitor lenacapavir have been described (e.g., M66I, Q67H/K/N, K70H/N/R/S, and/or N74D/H/K) after treatment failure in highly treatment-experienced individuals on functional monotherapy; however, no commercial capsid genotype resistance test is currently available Margot, et al. 2025. There is also no commercially available resistance test for the attachment inhibitor fostemsavir because of the broad diversity of envelope glycoprotein 120 and its effect on susceptibility to temsavir (the active metabolite), which has prevented the establishment of algorithms to assess resistance Schapiro, et al. 2025. Likewise, there is no commercially available resistance test for the attachment inhibitor ibalizumab Cluck, et al. 2024.
Table 3, below, lists indicated genotypic resistance tests based on HIV viral load.
| Abbreviations: ART, antiretroviral therapy; INT, integrase; PR, protease; RT, reverse transcriptase. | |
| Table 3: Genotypic Resistance Testing Based on Viral Load | |
| HIV RNA (Viral Load) | Indicated Genotypic Resistance Test |
| 0 to 500 copies/mL | HIV proviral DNA genotype (RT, PR, INT) or phenotype (tropism) |
| 500 to 1,000 copies/mL | HIV RNA genotype (RT, PR, INT) or phenotype (tropism) at assay amplification threshold; may use HIV proviral DNA test if nonamplifiable |
| ≥1,000 copies/mL | HIV RNA genotype if currently or recently (within 4 weeks) on ART; DNA proviral genotype may be considered for patients who are currently not taking ART but have in the past |
ART Changes to Address Drug Resistance
| RECOMMENDATIONS |
Changes to Address Drug Resistance
|
Abbreviations: 3TC, lamivudine; ART, antiretroviral therapy; ARV, antiretroviral medication; BIC, bictegravir; DRV, darunavir; DTG, dolutegravir; ETV, entecavir; FTC, emtricitabine; HBV, hepatitis B virus; INSTI, integrase strand transfer inhibitor; PI, protease inhibitor; RAM, resistance-associated mutation; TAF, tenofovir alafenamide; TDF, tenofovir disoproxil fumarate. |
Guiding Principles
Selection of an effective ART regimen for patients with preexisting or selected ARV drug resistance can be challenging but is achievable by following 4 guiding principles:
- Address the barriers to adherence that may have contributed to first-line treatment failure Schaecher 2013.
- Do not compromise treatment efficacy for convenience.
- Account for all RAMs that may have been transmitted or selected during prior treatment courses.
- Strive to construct the most tolerable and acceptable treatment regimen to suppress preexisting drug-resistant HIV effectively.
The ideal: The ideal ART regimen optimizes pharmacokinetics and adverse effect profiles, is easy to adhere to, and accounts for RAMs. One resource for assessing the effect of RAMs is the Stanford University HIV Drug Resistance Database. Importing RAMs into this algorithm allows clinicians to weigh the efficacy of different ARVs and avoid those with limited activity due to high resistance levels. It is crucial to review all previous genotypic and phenotypic resistance test results, to the extent possible, to identify any RAMs that have been present at any time during a patient’s treatment history. RAMs that may have been identified on historical resistance test reports that are not reported on subsequent testing should be considered to be archived within integrated HIV genomes. That is, these resistant strains remain dormant (latent) within long-lived CD4 cells and can reemerge during subsequent therapy that does not contain medications that remain active in their presence. Resistance mutations are not always consistently identified on repeated RNA or DNA genotype testing which may reflect sampling issues, fluxes in the dominant viral subpopulation due to selective pressure from treatment, or decay of the archived reservoir [D’Antoni, et al. 2024]. Therefore, constructing a composite genotype of all identified RAMs to account for any present or archived strains and reviewing responses to all prior ARV regimens may help in selecting subsequent ART regimens.
HIV-ASSIST offers a free online tool for selecting ART regimens based on HIV drug resistance mutations and comorbidities. Creating a fully suppressive treatment regimen is the goal, but HIV can evolve resistance to all existing classes of ARVs, especially in long-term survivors who were adherent to serial treatment intensifications as new agents were developed. Management of such cases requires expertise in identifying partially active agents that, when combined, can slow viral growth and fitness to replicate Buckheit 2004. For highly treatment-experienced patients with limited options, clinicians can search ClinicalTrials.gov for active studies of novel therapeutics for HIV, which may include monoclonal antibodies, long-acting agents, and agents with unique mechanisms of action and next-generation molecules.
Identifying Switch Options
Strains: In some cases of high-level multidrug-resistant virus with few evident treatment options in which a number of previously obtained genotypic or phenotypic test results are available, it is helpful to look at patterns of mutational sequences to identify HIV strains that may have been selected by past treatment sequences to construct regimens that have at least 2 drugs with activity for each strain. For example, there may be a genotype test result demonstrating 1 or more thymidine analog resistance mutations (TAMs) from prior zidovudine (ZDV) use along with non-nucleoside reverse transcriptase inhibitor (NNRTI) mutations from past efavirenz (EFV) use, but a subsequent genotype test result may show a nucleoside/nucleotide reverse transcriptase inhibitor (NRTI) RAM such as K65R selected by tenofovir (TFV) and PI mutations. An archive genotype test may show all of the NRTI, NNRTI, and PI mutations; however, interpretation of the sequences from serial past genotypes may clarify that these mutations may not all be present on any single strain, but rather an earlier strain that is susceptible to both PIs and INSTIs and a latter strain susceptible to NNRTIs and INSTIs. Therefore, a regimen of a PI/INSTI/NNRTI would provide 2 fully active drugs, 1 of which has a high genetic barrier, for both strains.
Potency and resistance barrier: Because of the variety of ARV therapeutic classes available and the availability of later-generation agents that are effective against virus otherwise resistant to older drugs within a class, multiple treatment options may remain after RAMs have developed. In these cases, potency and barrier to resistance should determine drug choices. Resistance barrier refers to the likelihood that a drug within a combination regimen will become resistant following treatment failure. Generally, agents with a higher barrier to resistance include BIC and DTG among the INSTIs, ritonavir-boosted DRV (DRV/RTV) among PIs, and etravirine (ETR) and doravirine (DOR) among NNRTIs. For example, a meta-analysis of 7 randomized clinical trials that included 1,686 treatment-naive and -experienced participants who used a once-daily boosted DRV regimen found that only 4 (0.2%) developed a PI or DRV RAM and only 1 (<0.1%) developed DRV resistance Lathouwers, et al. 2017. Including a drug with a high resistance barrier not only protects against development of RAMs after treatment failure but also reduces the likelihood that resistance to other drugs in the regimen will develop Luber 2005.
The effect of resistance barrier on viral suppression was illustrated in the SWITCHMRK trial, in which treatment-experienced participants who were virally suppressed on a high genetic barrier boosted PI-based regimen of RTV-boosted lopinavir (LPV/RTV) were randomized to continue their current regimen or switch to a raltegravir (RAL)-based regimen, an INSTI with a low genetic barrier, to assess effect on lipid control Eron, et al. 2010. Virologic control was not maintained to the same extent in those who switched to RAL as in those who continued LPV/RTV. This is in contrast to a switch study conducted in Kenya in which treatment experienced patients who were virally suppressed on boosted PI–containing regimens successfully maintained viral suppression after switching to the high genetic barrier, highly potent INSTI DTG Ombajo, et al. 2023; Cahn, et al. 2013.
Resistance barrier can be defined by the number of mutations that must be accumulated to incur resistance or the relative ease with which a mutation will emerge in the virus under selective pressure. Some mutations, such as the NRTI mutation K65R associated with TFV use, are rarely selected compared with others, such as the NRTI mutation M184V associated with 3TC or FTC use. Factors such as drug effectiveness, preexisting RAMs, and effect on viral growth capacity (fitness) can affect the relative ease of mutation selection during therapy Brenner and Coutsinos 2009.
The NADIA trial conducted in sub-Saharan Africa demonstrated the benefit of using a boosted PI or an INSTI with a high genetic barrier after NNRTI failure in individuals with NRTI resistance Paton, et al. 2022. Participants were randomized to receive DRV/RTV once daily or DTG once daily with either TDF/FTC or ZDV/3TC. At 96 weeks, DTG was noninferior to DRV/RTV, although 4% of participants developed DTG RAMs and none developed DRV RAMs on their respective treatments. Continuing TDF/FTC was superior to switching to ZDV/3TC despite nearly 58% of those assigned to the TDF/FTC arm having no predicted NRTI activity. The benefit of retaining TDF/FTC may be related to the low fitness of virus containing K65R and M184V mutations, as well as lower adherence due to twice daily dosing and poorer tolerability of ZDV. The D2EFT study, also conducted in sub-Saharan Africa, demonstrated the effectiveness of the combination of DTG plus DRV/RTV after failure with a regimen of 2 NRTIs plus 1 NNRTI. DTG plus DRV/RTV and DTG plus TDF/FTC or TDF/3TC were noninferior to 2 NRTIs plus DRV/RTV (the standard of care), and DTG plus DRV/RTV was found to be superior to the standard of care boosted PI regimen Matthews, et al. 2023.
Resistance to ARVs with a high genetic barrier, such as boosted PIs or second-generation INSTIs, is rare but can develop when other regimen components have limited activity and adherence is poor. In 2019, the World Health Organization began recommending DTG-based regimens as preferred first- and second-line treatment for all populations WHO 2019. The preferred regimen for low- and middle-income countries for first- and second-line treatment is TFV/3TC/DTG Kanters, et al. 2020. In the ACTG A5381 prospective cohort study conducted in Africa and Haiti among participants with HIV viral loads >1,000 copies/mL while on first-line NNRTI-based regimens (cohort 1, N = 44) or second-line PI-based regimens (cohort 2, N = 173), improvements in viral suppression <200 copies/mL (76% in cohort 1, 64% in cohort 2) at 24 months were less than anticipated Wallis, et al. 2024. Suboptimal suppression was associated with switches from failing second-line therapy (1% of participants in cohort 2 developed new DTG RAMs) and was likely due to poor adherence. Similar findings were reported from Malawi and Zambia Skrivankova, et al. 2024. Two years after routine, nonrandomized switching to DTG-based regimens, individuals who were virally suppressed at the time of switch had higher virologic control than those who were viremic, and there was low development of DTG RAMs overall (4% of 45 amplifiable sequences from participants with HIV viral loads >1000 copies/mL had DTG RAMs).
In Kenya, where DTG-based therapy was adopted as the standard in 2017, a review of resistance patterns in 190 samples collected from January to March 2023 from individuals with HIV viral loads >200 copies/mL (41 taking DTG-based regimens as first-line treatment, and 149 taking DTG-based regimens as second- or third-line treatment) found 18.6% with DTG RAMs (in 8.3% and 22.6%, respectively) Kingwara, et al. 2024. A reference laboratory in Mexico reported that the most common INSTI RAMs identified in samples collected from October 2021 to September 2023 were Q148H, G140S, and R263K, and viral loads <5,000 copies/mL were observed in individuals taking failing regimens with virus containing R263K, suggesting a fitness disadvantage for the mutant strain Juárez-González, et al. 2024. The R263K and N155H INSTI RAMs have also been found to impair reverse transcription, which may account for the impaired fitness of breakthrough virus Ratouit, et al. 2024.
Table 4, below, lists ARVs categorized by their level of genetic barrier to resistance.
Notes:
|
||
| Table 4: Antiretroviral Medications by Level of Genetic Barrier to Resistance [a,b] | ||
| Low Resistance (single mutation, common) |
Intermediate Resistance (1 or 2 mutations, common) |
High Resistance (>2 mutations, rarer) |
|
|
|
Selecting the most effective ART regimen to suppress an HIV strain with established RAMs requires an understanding of the available treatment options, appreciation of cross-class resistance among related agents, and avoidance of combinations that have not demonstrated potency in clinical trials.
Available ARV classes: Box 1, below, lists the 7 currently available classes of ARVs in the order of their position in interruption of the HIV life cycle.
| Box 1: Antiretroviral Medication Classes in Order of Position in Interruption of HIV Life Cycle |
|
Cross-resistance within ARV classes: Although an ARV class may include several drugs, they often share resistance profiles, which may limit options for a switch within a class. For example, among NRTIs, FTC and 3TC share complete resistance. Some drugs within a class can retain activity after failure of related compounds. For example, EFV treatment may fail with the development of the K103N mutation, but rilpivirine (RPV), DOR, and ETR would still retain activity. Drugs developed later that have higher resistance barriers are referred to as second (or later) generation and include ETR (NNRTI), DTG and BIC (INSTIs), and DRV and TPV (PIs). The International Antiviral Society-USA has developed tables of the major and minor mutations associated with ARV resistance that illustrate the overlap across drugs within classes. Major mutations are those with a more profound effect on virus susceptibility. In general, HIV resistance develops stepwise, with the primary mutation appearing first. This mutation allows the virus to survive and continue to replicate under the pressure of drug treatment. If HIV is not resuppressed, additional mutations will emerge that increase viral growth fitness and the potential for cross-class resistance. For example, the initial RAM usually selected by RPV is E138K, which would have little effect on other NNRTIs Hayashida, et al. 2016. Understanding the unique patterns of resistance selection by drugs and responding rapidly to virologic failure can be useful in selecting the most effective ART options.
HIV resistance evolves in a predictable manner over time, with drugs with a lower resistance barrier affected first, allowing viral replication and further selection pressure to reduce effectiveness of other drugs in the regimen and enhance growth capacity. RAMs can evolve rapidly; for example, half of a population of virus will become resistant to 3TC (from selection of a single mutation) within 5 weeks of 3TC monotherapy Feder(a), et al. 2021. Resistance to currently preferred combinations takes longer and depends on several factors, including resistance barrier, regimen potency, medication exposure, and viral load, making it unlikely that resistance will emerge while resistance testing results are pending. That time affords the opportunity to address adherence barriers that might be contributing to poor viral response.
Patients who have viral breakthrough or suppressed viral load despite having virus that is resistant to a single therapeutic class can still have options for simplified therapy, including single-tablet regimens (see Table 5, below). To adopt this approach, therapy regimens must be based on a complete history of previous treatment failures, resistance testing, and tolerability.
| Abbreviations: ART, antiretroviral therapy; ARV, antiretroviral drug; BIC, bictegravir; COBI, cobicistat; DOR, doravirine; DRV, darunavir; DTG, dolutegravir; ETR, etravirine; FTC, emtricitabine; FTR, fostemsavir; IBA, ibalizumab; INSTI, integrase strand transfer inhibitor; LEN, lenacapavir; MVC, maraviroc; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside/nucleotide reverse transcriptase inhibitor; PI, protease inhibitor; RAM, resistance-associated mutation; RPV, rilpivirine; RTV, ritonavir; TAF, tenofovir alafenamide; TPV, tipranavir.
Notes:
|
|
| Table 5: ART Options After First-Line Treatment Failure With Single-Class Drug Resistance [a,b] | |
| Failed First-Line Regimen Drug Classes | Classes and Medication Options for Switch |
| 2 NRTIs + 1 NNRTI [a] |
|
| 2 NRTIs + 1 PI [a] |
|
| 2 NRTIs + 1 INSTI [a] |
|
| Multiclass |
|
Alternative strategy: It has been a general principle of ART strategy to include new medication classes when constructing second-line and subsequent ART regimens following virologic failure and drug resistance selection. In particular, the addition of high genetic barrier agents, such as a PI (boosted with RTV or cobicistat [COBI]) or a second-generation INSTI, can improve successful viral suppression.
An alternative or complementary strategy is to include later-generation agents within a class that may retain activity against the resistant strain, such as the boosted PIs DRV or TPV; the NNRTI ETR, and in some instances RPV (with K103N only) or DOR; and the INSTIs DTG and BIC. For example, in the DUET 1 and 2 trials, which enrolled adults on failing therapy with NNRTI and PI resistance mutations, the combination of a second-generation NNRTI (ETR) and boosted PI (DRV/RTV) achieved sustained viral suppression for 96 weeks Katlama, et al. 2010. TFV may retain activity due to its barrier to resistance related to viral hindrance from selecting its primary resistance mutation K65R (discussed above). Likewise, 3TC has been demonstrated to retain clinical activity (as discussed below) even in the presence of its signature drug resistance mutation M184V Ciaffi, et al. 2017. In the VIKING-3 study, a twice-daily oral dose of DTG 50 mg with an optimized background regimen was used in 183 treatment-experienced participants with a history of INSTI-resistant HIV and few treatment options. Viral suppression (HIV RNA <50 copies/mL) response was relative to the presence of the Q148 mutational pattern: no Q148 (79% of 126 participants); Q148 plus 1 other RAM (58% of 36 participants); Q148 plus ≥2 other RAMs (24% of 21 participants) Castagna, et al. 2014.
| KEY POINT |
|
How Many Active Drugs Are Enough?
The traditional answer is 3 (see below for the exception). Based on this principle, ARVs are added to a regimen until it accumulates the equivalent of 3 fully active drugs. New classes of therapy add a count of 1 because there is no preexisting resistance. Partially active agents may add only a fraction depending on their relative resistance (partial, low-level). Therefore, regimens can become fairly complex.
Genotypic susceptibility score: The activity of a second-line or subsequent ART regimen can be predicted by its genotypic susceptibility score (GSS), a rating system in which each active drug (based on the Stanford University HIV Drug Resistance Database genotypic resistance interpretation system) contributes a full (1) or partial (fraction) to the score Gonzalez-Serna, et al. 2017. Improved viral suppression rates have been demonstrated to correlate with increased GSS in short-term follow-up (16 to 24 weeks) after regimen switches Anderson, et al. 2008. A limitation is that GSS assigns an equal score to medications with low and high drug potency.
Typically, the GSS is calculated by adding up mutations or using the Stanford University HIV Drug Resistance Database to identify potentially active agents. However, for some medications that may be considered for highly treatment-experienced patients, such as DRV de Meyer, et al. 2008; de Meyer, et al. 2005, TPV/RTV Marcelin, et al. 2008, and ETR Vingerhoets, et al. 2010, a weighted genotypic score in which certain mutations have a greater effect than others in achieving viral suppression may be used. These algorithms can be useful in interpreting genotypes for cases in which more complicated regimens may be needed. In addition, therapeutic drug monitoring has been used to assess a genotypic inhibitory quotient to represent the extent to which the measured trough drug concentration exceeds the amount needed to suppress virus based on the weighted GSS Gonzalez de Requena, et al. 2011. This method demonstrates the value of weighted scores in interpreting resistance in highly treatment-experienced patients, but it is not readily available for clinical practice.
2-NRTI backbone: An established practice based on the evolution of ART has been to start building regimens on a “backbone” of 2 NRTIs and adding a third, fourth, or additional agent as needed. However, the combination of DRV/RTV, ETR, and RAL without NRTIs among triple-class-experienced participants whose previous ART failed demonstrated significant long-term activity (88% suppression at 96 weeks) in an open-label, multicenter clinical trial in Europe and rural treatment sites in the United States where monitoring was more difficult Ebers, et al. 2017; Fagard, et al. 2012.
Some studies indicate that retention of NRTIs in constructing regimens after virologic failure contributed additional benefit even when resistance assays predicted limited residual activity Scherrer, et al. 2011. The presence of the M184V mutation, in particular, which contributes high-level resistance to 3TC and FTC, has properties that may be advantageous in a second-line regimen, including improving the susceptibility of coadministered NRTIs (such as TFV) even when resistance mutations are present, reducing viral fitness to replicate, and decreasing the rate of viral mutation by improving the fidelity of the HIV reverse transcriptase and making it less error prone Wainberg 2004. A randomized clinical trial with treatment-experienced participants, however, demonstrated that when an ART regimen could be constructed that had a phenotypic susceptibility score >2 (i.e., containing at least 2 fully active agents not counting NRTIs), omitting NRTIs was noninferior to adding NRTIs with regard to viral suppression rates (HIV RNA <50 copies/mL) at week 96 Gandhi, et al. 2020; Tashima, et al. 2015. Therefore, if a fully active regimen (at least 2 fully active agents, including at least 1 with a high genetic barrier such as a PI or an INSTI) can be constructed for a highly treatment-experienced patient without including an NRTI, there would be no need to add one. However, if it is possible to construct only a partially active regimen, then inclusion of 1 or 2 NRTIs based on their unique characteristics may be beneficial.
The results of the BENCHMRK-1 and BENCHMRK-2 clinical trials of the INSTI RAL demonstrate some of the key principles for constructing ART regimens in a highly treatment-experienced patient with multiclass drug-resistant virus Eron, et al. 2013. The study recruited participants who were RAL-naive with HIV resistant to ARVs from 3 or more classes and randomized them to receive RAL or placebo added to an optimized background therapy chosen from all available treatment options at that time. The results demonstrated that use of the new class of drug (INSTI) led to higher viral suppression rates at week 156 than placebo (51% vs. 22% with HIV RNA <50 copies/mL). It also demonstrated that inclusion of the fully active PI DRV in the optimized background regimen improved response to 72% and the new class fusion inhibitor enfuvirtide to 79% viral suppression. The optimized background therapy in the study was rated by a GSS in which 0 equals no fully active agents, 1 equals 1 fully active agent, 2 equals 2 fully active agents, and ≥3 equals 3 or more fully active agents in the background therapy. The addition of RAL improved viral response for all GSS background regimens, with additional benefit diminishing as the GSS score increased Eron, et al. 2013.
Three fully active ARVs may not be needed in a second-line or subsequent regimen if 1 of the agents is fully active with a high genetic barrier. In a large cohort study, patients whose NRTI/NNRTI-based first-line therapy responded equally well to RTV-boosted PI-based therapy regardless of the number of active NRTIs used and the overall GSS of the regimen Waters, et al. 2013. The second-generation INSTI DTG plus 2 NRTIs was demonstrated in a randomized trial to have a 48-week viral suppression rate (84%) superior to that of RTV-boosted LPV (70%) in resource-limited settings among participants who had experienced virologic failure on 2 NRTI/1 NNRTI-based therapy in which the GSS of the NRTI background regimen was <2 among 81% of the participants Aboud(a), et al. 2019. Similarly, the VISEND study from Zambia confirmed the effectiveness of using DTG, an INSTI with a high genetic barrier, with recycled NRTIs Mulenga, et al. 2022.
Single-Tablet or Once-Daily Regimen After Virologic Failure
In the past, virologic failure often required construction of increasingly complex ART regimens, including use of medications dosed twice daily, which exacerbated the adherence problems that were frequently the cause of the initial treatment failure. Agents with a high resistance barrier can often be used to anchor second-line and later ART regimens and make once-daily and, at times, single-tablet regimens viable options.
In the ODIN trial, among participants with a history of ART failure (54% of whom had PI experience, including 28% with prior use of 2 or more PIs) and no primary DRV resistance mutations (V11I, V32I, L33F, I47V, I50V, I54L, I54M, T74P, L76V, I84V, and L89V), no difference was found in virologic suppression between use of once- or twice-daily DRV/RTV Cahn, et al. 2011. In another study, adults who were virally suppressed on a TAF/FTC/DTG regimen successfully maintained viral suppression after switching to TAF/FTC/BIC stratified by known or suspected prior NRTI resistance (K65R or ≥3 TAMS vs. other NRTI RAMs vs. no NRTI RAMs) Sax(a), et al. 2020. Similarly, viral suppression was maintained among Black participants after switching from regimens of 2 NRTIs plus a third agent to TAF/FTC/BIC, regardless of prior drug resistance (10% with M184V/I, 7% with TAMs, 21% with NNRTI resistance, and 13% with PI resistance) Andreatta, et al. 2020. Participants whose previous resistance test results demonstrated the presence of K65R/E/N, ≥3 TAMs, T69 insertion, or INSTI RAMs were excluded from the study.
In the 2D study, in which treatment-experienced participants who had a history of HIV drug resistance to at least 2 ARV classes and retained full susceptibility to DRV and DTG and were virally suppressed on a 3-drug or more ART regimen were randomized 1:1 to switch to the 2-drug once-daily regimen of DRV/COBI plus DTG or maintain standard of care (median 5 tablets daily), there were no virologic failures in the 2-drug arm Santos, et al. 2023. Inclusion of fully active agents with a high genetic barrier to resistance can be an option for regimen simplification to maintain viral suppression and avoid accumulation of additional RAMs.
Agents for Use in Highly Treatment-Experienced Patients
As noted above, some patients, usually those who have had HIV for many years and have been at least partly adherent to multiple sequential nonsuppressive therapies or younger individuals who acquired HIV perinatally and, similarly, used multiple sequential therapies, have developed multiclass drug-resistant virus, limiting options for constructing a fully active ART regimen from the 4 major drug classes alone. The proportion of such patients has declined over time and they currently represent less than 1% of people with HIV in care, but these patients also present unique treatment challenges Bajema, et al. 2020.
The viral reservoir consists of an archive of wild-type and heterogeneous viral variants generated since the time of infection in response to immune pressure, selected by previously used nonsuppressive regimens and through transmission Noe, et al. 2005. Drugs with associated RAMs identified on prior resistance testing or on archive DNA genotyping may still be used in regimens for highly treatment-experienced individuals, as these drugs will be active against susceptible subpopulations. To construct regimens with the equivalent of 3 fully active agents (or at least 2 active drugs with 1 that is fully active and has a high resistance barrier, such as a boosted PI or second-generation INSTI), the use of novel drug classes described below may be necessary.
Ibalizumab (IBA): IBA is the first monoclonal antibody therapy approved by the U.S. Food and Drug Administration (FDA) for the treatment of HIV. IBA attaches to the CD4 binding site for HIV envelope glycoprotein 120 (gp120), inhibiting viral attachment. After the initial loading dose (2,000 mg intravenous [IV] push or 30-minute IV infusion), the medication is administered intravenously every 2 weeks (800 mg) and may be given via 30-second IV push or 15-minute IV infusion. A phase 3 study of highly treatment-experienced participants (>90% with NRTI, NNRTI, and PI resistance and 68% with resistance to at least 1 agent per class) demonstrated that 83% achieved a 0.5-log and 60% a 1.0-log reduction in viral load after 7 days of effective monotherapy and 43% had a viral load <50 copies/mL at week 25 Chahine and Durham 2021; Emu, et al. 2018. Of note, 9 of 10 participants with virologic failure or rebound (25% of participants) had HIV that demonstrated reduced IBA susceptibility, indicating a low resistance barrier to this agent. When taking IBA combined with at least 1 other fully active agent, 71% of participants achieved a viral load <50 copies/mL, and when combined with at least 2 fully active drugs, 56% achieved viral loads <50 copies/mL at week 25. Responses were better if the fully active agent was DTG; 75% and 78% of participants achieved viral suppression <50 copies/mL when DTG was the only or 1 of 2 fully active agents in the regimen Chahine and Durham 2021; DeJesus, et al. 2020. As ibalizumab will be a single component of a mixed oral/injectable regimen, it is crucial that adherence to the other agents in the combination be strict because the risk of monotherapy with the potential for development of resistance is high Beccari, et al. 2019.
Fostemsavir (FTR): FTR has been approved by the FDA for treatment of multidrug-resistant HIV. FTR functions as a CD4 attachment inhibitor by binding to HIV gp120. The registrational study included a randomized arm (for optimized background therapy with at least 1 other active agent) and a nonrandomized arm (when no additional fully active agent was available) Kozal, et al. 2020. The randomized arm included an 8-day effective monotherapy period in which 68% and 50% of participants achieved 0.5-log and 1.0-log reductions in viral load, respectively. In the randomized arm, 53% achieved viral load suppression (HIV RNA <40 copies/mL) by week 24, with poorer responses among those with viral loads >100,000 copies/mL or CD4 counts <20 cells/mm3 (35%). In the nonrandomized cohort, 37% achieved viral load suppression (HIV RNA <40 copies/mL) at week 24, with an improved response among 15 patients (53%) who also received IBA, which was allowed per study protocol.
Maraviroc (MVC): MVC is an oral attachment inhibitor that blocks HIV gp120 from binding to the CCR5 coreceptor on the T-cell surface following CD4 binding. HIV tropism is dynamic, and most transmitted HIV is CCR5 (macrophage, or M) tropic. However, over time, viral phenotype may, during the course of uncontrolled viremia, develop the capacity to bind to an alternative (or additional) coreceptor CXCR4 (T-cell, or T-tropic). This shift in tropism occurs independently of ARV pressure but coincides with a longer time of infection and higher levels of treatment experience Mosier 2009. Therefore, when a novel, fully active agent may be needed, MVC as a purely CCR5-active agent may be less likely to contribute to treatment response. Before switching to a regimen that includes MVC, a tropism assay that demonstrates only CCR5 (not dual or X4-tropic) virus in the population should be confirmed. RNA tropism can be assessed if the plasma viral load is ≥500 copies/mL, and DNA tropism assays may be used when viral loads are lower or undetectable. However, historical tropism results may not be reliable if a period of viral replication ensued after the assay was obtained, so when viremia is present, a tropism assay should be performed as soon as possible proximate to the planned use of MVC. In 2 randomized, placebo-controlled clinical trials, participants with R5-tropic virus who had been treated with or had resistance to agents in 3 ARV classes who received MVC in addition to an optimized background therapy had significantly improved viral suppression rates and improvement in CD4 cell counts at 48 weeks Gulick, et al. 2008.
Lenacapavir (LEN): LEN is a long-acting, injectable capsid inhibitor administered subcutaneously every 6 months after oral lead-in doses. The capsid protein protects the viral RNA, and inhibition of its function can affect early (uncoating, reverse transcription), mid (nuclear entry), and late (assembly) stages in the HIV lifecycle Carnes, et al. 2018.
Analysis of week 52 results from the phase 2/3 CAPELLA study of highly treatment-experienced participants with HIV found that 83% maintained a viral load of <50 copies/mL and 86% maintained a viral load of <200 copies/mL (randomized cohort) when LEN was used with optimized background ART Ogbuagu(a), et al. 2023. At enrollment, 47% of participants had resistance to all 4 ARV classes, 54% to INSTIs, 42% to all PIs, and one-third to IBA and FTR Segal-Maurer, et al. 2022. Further, 67% of participants maintained viral suppression despite having no fully active agent in their optimized background regimen, 79% maintained viral suppression with 1 fully active agent, and 94% maintained it with 2 fully active agents. Among 8 participants with RAMs at virologic failure, 1 died at week 11, 3 had no fully active background agent, and 4 had inadequate adherence to the background therapy. Subgroup analysis at 104 weeks identified 12 participants (17%) with no fully active ARVs in their optimized background regimen (OBR), including 5 with no partially active agents Ogbuagu, et al. 2024. Three-quarters of participants with LEN as the only fully active agent (9/12) maintained viral suppression (1 suppressed with OBR change at week 25, and 2 maintained low-level viremia throughout), and 3 developed LEN resistance, although 2 of the 3 were virally suppressed at week 104. In clinical studies of mostly treatment-experienced individuals with HIV who received LEN, capsid inhibitor mutations were identified in 19 of 258 participants (7%) Demirdjian, et al. 2024. Subgroup analysis found no differences in response rate at week 52 based on age (<50 or ≥50 years), sex assigned at birth (male or female), race (Black or non-Black), baseline CD4 count (<200 or ≥200 cells/mm3), baseline viral load (≤100,000 or >100,000 copies/mL), presence of baseline INSTI resistance, or inclusion of specific agents in the optimized background regimen (i.e., DRV, DTG, IBA, or FTR) Ogbuagu(b) 2023. The most common adverse effects associated with LEN were diarrhea, nausea, and injection site reactions, and 1% of participants discontinued treatment because of toxic effects.
LEN is a moderate cytochrome P450 3A inhibitor and may interact with coadministered ART and other medications (see package insert). After subcutaneous dosing, LEN can persist in the blood for more than 12 months at diminishing concentrations; therefore, if LEN is discontinued, a fully suppressive ART regimen should be initiated within 28 weeks after the final injection FDA 2024. Currently there is no commercially available capsid inhibitor resistance assay. As LEN will be a single component of a mixed oral/injectable regimen, it is crucial that patients maintain strict adherence to the other agents in the combination because of the high risk of monotherapy with the potential for development of resistance Wirden, et al. 2024.
ART Changes for Adverse Effects, Drug-Drug Interactions, or Pregnancy
| RECOMMENDATIONS |
Changes to Address Adverse Effects
Changes to Address Drug-Drug Interactions
Changes Due to Pregnancy
|
Abbreviations: 3TC, lamivudine; ART, antiretroviral therapy; ARV, antiretroviral medication; COBI, cobicistat; DHHS, U.S. Department of Health and Human Services; ETV, entecavir; FTC, emtricitabine; HBV, hepatitis B virus; RTV, ritonavir; TAF, tenofovir alafenamide fumarate; TDF, tenofovir disoproxil fumarate. |
It is imperative that clinicians review the appropriateness of their patient’s ART regimen at every visit in the context of updated laboratory testing results, medication reconciliation, and any new diagnoses. In addition, clinicians should remain informed about the prescribed ART regimen’s adverse effects and drug-drug interaction profiles.
Changes to Address Adverse Effects
Table 6, below, lists common adverse effects associated with ARVs.
| Abbreviations: CNS, central nervous system; eGFR, estimated glomerular filtration rate.
Notes:
|
|
| Table 6: Common Adverse Effects Associated With Antiretroviral Medications | |
| Drug | Adverse Effect(s) |
| Nucleoside/Nucleotide Reverse Transcriptase Inhibitors | |
| Abacavir [a] | Cardiovascular disease, hypersensitivity |
| Didanosine | Mitochondrial toxicity, lipodystrophy, lactic acidosis |
| Stavudine | Mitochondrial toxicity, lipodystrophy, lactic acidosis |
| Tenofovir alafenamide | Weight gain, increased lipids Mallon, et al. 2021 |
| Tenofovir disoproxil fumarate | Proximal renal tubule injury, decrease in bone mineral density |
| Zidovudine | Mitochondrial toxicity, lipodystrophy, lactic acidosis |
| Non-Nucleoside Reverse Transcriptase Inhibitors | |
| Doravirine | CNS effects |
| Efavirenz | Hepatotoxicity, vitamin D deficiency, CNS effects, skin reactions, depression, morning somnolence |
| Nevirapine | Hepatotoxicity, hypersensitivity |
| Rilpivirine | CNS effects, skin reactions, effects on the measure of eGFR |
| Protease Inhibitors Tsiodras, et al. 2000 | |
| Class effect [b] | Increased cholesterol [c], increased triglycerides [c], increased glucose, lipodystrophy |
| Atazanavir | Nephrolithiasis, renal insufficiency, hyperbilirubinemia |
| Darunavir | Cardiovascular disease, skin reactions |
| Lopinavir/ritonavir | Cardiovascular disease Ryom, et al. 2018 |
| Integrase Strand Transfer Inhibitors | |
| Class effect [b] | Weight gain Sax(b), et al. 2020 |
| Bictegravir | Effects on the measure of eGFR |
| Dolutegravir | CNS effects Yombi 2018; Hoffmann, et al. 2017, effects on the measure of eGFR |
| Elvitegravir/cobicistat | Increased lipids, effects on the measure of eGFR |
Chronic comorbid conditions, such as diabetes, cardiovascular disease, osteoporosis, chronic kidney disease, and dyslipidemia, should influence ART choices. In addition, some drugs, especially protease inhibitors (PIs), may cause unfavorable lipid changes. Although no consensus exists, some studies have shown an increased risk of cardiovascular events with abacavir use Jaschinski, et al. 2023; Dorjee, et al. 2018; Sabin, et al. 2018. Exploratory analysis of the REPRIEVE trial on the impact of statins on major adverse cardiovascular events among people with HIV found current and former use of abacavir (ABC) was associated with higher incidence of major adverse cardiovascular events even though participants were at low risk for cardiovascular disease and had normal kidney function Fichtenbaum, et al. 2024. Given this evidence, ABC should be avoided or used with caution, particularly in patients with multiple cardiac risk factors or known coronary heart disease, and alternative regimens considered. Decisions about treatment options should be made on an individual basis by practicing shared decision-making with patients, sharing current evidence and carefully weighing potential risks and benefits. In situations in which ABC continues to be used (e.g., patient declines to change regimen), extra vigilance in managing cardiovascular risk factors is warranted.
Patients with preexisting kidney disease or osteoporosis may experience worsening of both over time with TDF, given its association with renal insufficiency (through proximal renal tubular dysfunction) and bone mineral density loss. TAF has demonstrated less effect on bone density and renal function parameters than TDF Wang, et al. 2016, although it is also associated with increased total cholesterol and the potential for weight gain Squillace, et al. 2020. Switching from TDF to TAF has been associated with a significant increase in triglyceride levels, total cholesterol, and high-density lipoprotein (HDL) cholesterol, but no significant changes in low-density lipoprotein cholesterol and total cholesterol/HDL ratio. However, calculated cardiovascular risk increased after switch from TDF- to TAF-based therapy Plum, et al. 2021.
A multicenter, open-label study of 1,443 adults with a glomerular filtration rate (GFR) >50 mL/min on stable TDF-containing ART regimens who were randomized 2:1 to switch to TAF or remain on TDF demonstrated equivalent maintenance of viral suppression with improved bone mineral density at the hip and spine and improved GFR in the TAF arm at 48 weeks Mills, et al. 2016. These findings were similar to those reported in a double-blind, multicenter, placebo-controlled, noninferiority trial of 630 virally suppressed adults taking TDF/FTC/rilpivirine (RPV) who were randomized 1:1 to switch to TAF/FTC/RPV or remain on current therapy Orkin, et al. 2017; viral suppression was found to be noninferior and similar adverse effects were observed between the arms at 48 weeks.
Weight gain after ART initiation, especially with integrase strand transfer inhibitor (INSTI)-based regimens, PI-based regimens being intermediate and non-nucleoside reverse transcriptase inhibitor (NNRTI)-based regimens being less likely to have this association, has been a focus in recent reports Sax(b), et al. 2020. The inclusion of TAF as a component of an INSTI-based regimen has been shown to have a stronger link with weight gain Venter, et al. 2019. In a large, diverse U.S. cohort of people with HIV, a switch from TDF to TAF was associated with weight gain immediately after the switch, regardless of the core ART class or agent, suggesting an independent effect of TAF on weight gain Mallon, et al. 2021; Surial, et al. 2021. In the PASO-DOBLE study, which examined switches from complex suppressive ARV regimens to either DTG/3TC or BIC/TAF/FTC, greater weight gain was observed after switch to the TAF-containing regimen across subpopulations of sex, age, race, prior AIDS diagnosis, and baseline ART Tiraboschi, et al. 2025. The mechanism(s) underlying this association are under investigation.
To date, no data demonstrate that switching the ART regimen would reverse weight gain. The DEFINE study did not demonstrate weight reduction at 24 weeks in 103 participants with either early or delayed switch from TAF/FTC plus an INSTI to TAF/FTC/DRV/COBI Anderson, et al. 2024. The potential for weight gain and monitoring of weight gain should be discussed with patients initiating INSTIs. Weight gain is variable and may be managed in some people without ART modification. However, after discussion of these findings with their patients, clinicians may decide to switch ART because of this adverse effect.
The PROBE 2 trial examined switching to a 2-drug regimen of RPV plus darunavir/COBI from a fully suppressive 3-drug regimen of 2 nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs) plus an NNRTI, an INSTI, or an RTV-boosted PI to avoid potential NRTI toxic effects. Participants had no baseline NNRTI or PI resistance-associated mutations (RAMs) and did not have chronic HBV infection Maggiolo, et al. 2021. Half of participants were randomized to switch immediately (early) and half at week 48 (late), allowing a comparison with standard of care (n = 80 in each arm). At week 48, viral suppression <50 copies/mL was maintained in 87.5% of participants in the early switch arm (12.5% missing data) and 94.8% in the late-switch arm (2.6% missing data; noninferiority), and no virologic failures occurred in the early switch group. Although simplification achieved favorable virologic outcomes, lipids increased in the participants switched from TDF-containing regimens, but no increases in body weight were noted.
Many adverse effects may be shared across a class of drugs because of shared mechanisms of action and metabolic pathways; therefore, switches due to adverse effects may require a change to a different therapeutic class. A study of 415 adults older than 50 years with a Framingham cardiovascular risk of 10% or higher who were virally suppressed on a PI-containing regimen and randomized to early versus deferred switch to a dolutegravir (DTG)-containing regimen demonstrated improvement in the lipid profile in both arms after the switch Gatell, et al. 2019. Unfortunately, the study was not powered to show an effect on cardiovascular disease. Switching ART alone may not be sufficient to reduce cardiovascular disease risk, and the addition of lipid-lowering therapy may be indicated with or without switching Palella, et al. 2014. Insufficient data are available on the effect on weight gain when switching INSTIs to other ARV classes; clinical trials are underway that may provide evidence for guidance on this issue.
If a switch of ART regimen is indicated because of diminished renal function, prescribers should be aware that certain ARVs may alter the assessment of creatinine clearance. COBI, DTG, bictegravir (BIC), and, to a lesser extent, RPV have been associated with decreased creatinine secretion, leading to a slight rise in serum creatinine levels without a concomitant decline in GFR. A consensus statement from Australia recommends that serum creatinine levels be checked 1 month after initiation of these agents to establish a new baseline measurement Holt, et al. 2014. However, no data suggest this approach alters clinical management. Small studies show that estimation of GFR with cystatin C measurements may be more accurate in patients taking agents that affect creatinine secretion; this assay may be used if a more refined assessment of GFR is needed Galizzi, et al. 2018; Yukawa, et al. 2018.
Changes for Drug-Drug Interactions
Pharmacokinetics: A thorough search for drug-drug interactions should be performed whenever an ART regimen is initiated or changed or new medications are added to treat concomitant conditions. Drug classes that commonly cause pharmacokinetic interactions with ARVs include:
- Statins and other lipid-lowering and cardiovascular medications
- Inhaled and intra-articular corticosteroids
- Select psychotropics
- Narcotics and other sedatives
- Anticoagulants (factor Xa inhibitors) and antiplatelet agents (clopidogrel)
- Alpha-adrenergic blocking drugs to manage benign prostatic hyperplasia
- Phosphodiesterase inhibitors used for erectile dysfunction or pulmonary hypertension
- Antacids, proton pump inhibitors, and H2 blockers
- Anticonvulsants
- Rifampin/rifabutin (see DHHS Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents With HIV > Tuberculosis/HIV Coinfection)
- Recreational drugs (ketamine; benzodiazepines; crystal meth; 3,4-methylenedioxy-methamphetamine [MDMA]; mephedrone)
- PIs and NNRTIs, when combined
Most of these interactions are associated with ART regimens containing RTV or COBI. These agents are pharmacokinetic inhibitors of cytochrome P450 3A (CYP3A), a major enzyme system involved in most drug metabolism Lynch and Price 2007. The INSTIs BIC and raltegravir do not cause and are not affected by CYP3A interactions. CYP3A partly metabolizes DTG, and a coadministered inducer may reduce its levels. The NNRTIs doravirine (DOR) and RPV and the CCR5 antagonist maraviroc are substrates for CYP3A, and their levels may be affected by the concomitant use of an inducer or inhibitor. Etravirine (ETR), a second-generation NNRTI that may be useful for patients with NNRTI drug resistance, is an inducer of CYP3A and UGT1A1 and may reduce the levels of coadministered DTG Rathbun and Liedtke 2010. Use of DOR or RPV in place of ETR, if active, may avoid this interaction (see guideline section ART Changes to Address Drug Resistance > Identifying Switch Options > Cross-resistance within ARV classes). Therefore, when changing an ART regimen, it is important to assess drug-drug interactions not only between ARVs and concomitantly used medications but also within the ART regimen itself. Additional resources to assess ART drug-drug interactions include the University of Liverpool HIV Interaction Checker and the DHHS HIV guidelines.
Antacids are one common drug class responsible for interactions that could lead to subtherapeutic ARV concentrations. The NNRTI RPV and the PI atazanavir require an acidic gastric environment for optimal absorption, and concomitant use of antacids can lead to virologic failure. Additionally, a history of bariatric surgery would likely influence ART choices, given the need to crush pills for up to 3 months post-surgery and the possibility of poor absorption of extended-release medications Cimino, et al. 2018. Divalent cations, commonly found in multivitamins, can bind to and reduce the absorption of certain INSTIs. Phosphate-binding resins (e.g., sevelamer) used in end-stage renal disease may interfere with the absorption of many medications, including ARVs, which should be taken at least 1 hour before or 3 hours after the resin.
Complementary and herbal therapies, health supplements, minerals, and vitamins can also cause drug-drug interactions that may affect concentrations of ARVs Bordes, et al. 2020. A thorough accounting of all coadministered drugs, including over-the-counter and herbal remedies, should be conducted before prescribing ART and periodically during therapy or in the event of unexplained virologic failure. It is also appropriate to assess drug-food interactions, as some ARVs have food restrictions. Food can affect the rate and extent of ART absorption or alter the acid milieu of the gastrointestinal tract, which may affect effectiveness AIDSmap 2023; University of Liverpool 2016.
Prolonged viremia attributable to adverse pharmacokinetic drug-drug interactions can lead to the development of RAMs and potential cross-resistance among ARVs within the same class. Genotypic resistance testing should be considered to assess the effect of emergent RAMs on continued or reconfigured ART regimens.
If ART is changed and the new regimen includes or removes a pharmacokinetic inhibitor (e.g., RTV or COBI) or inducer (e.g., efavirenz), an assessment must be made of chronic coadministered medications whose metabolism may be affected. The addition or removal of pharmacokinetic “boosters” or “inducers” can cause adverse effects associated with elevated exposure or withdrawal of concomitant medication. However, because the only change made is the ART regimen, adverse effects may be falsely attributed to the new regimen rather than the need for dose adjustment or modification of the coadministered medication.
| KEY POINT |
|
Changes for Pregnancy
Patients of childbearing potential should be assessed for pregnancy status or plans to become pregnant (see DHHS Recommendations for the Use of Antiretroviral Drugs During Pregnancy and Interventions to Reduce Perinatal HIV Transmission in the United States).
Preliminary data suggested an increased rate of neural tube defects (NTDs) in a clinical trial in Botswana among infants born to mothers using DTG at the time of conception. The latest available data, through April 2020, show that the rate of infant NTDs with maternal DTG-based ART use at conception (0.19%) is not significantly greater than for infants exposed to non-DTG-based ART at conception (0.11%). Additionally, studies conducted in populations in the United States where folate supplementation is common did not demonstrate an excess in NTDs with use of DTG at conception APR 2024; DHHS 2024; Zash, et al. 2022. The current DHHS guideline recommends DTG as a preferred ARV at all stages of pregnancy.
People with HIV who are pregnant or planning a pregnancy may require ART modification because of pharmacokinetic factors Gilbert, et al. 2015. The efficacy of 2-drug ART in pregnancy has not been established; if a patient who is stable on 2-drug ART becomes pregnant, it may be appropriate to consider a switch to a preferred 3-drug regimen or the addition of a third ARV during pregnancy. Patients with viral suppression on a COBI-containing ART regimen should consider switching to an alternative regimen or be monitored closely for virologic breakthrough during pregnancy.
ART Changes for Regimen Simplification
| RECOMMENDATIONS |
Changes for Regimen Simplification
|
Abbreviations: ART, antiretroviral therapy; CAB/RPV LA, long-acting cabotegravir and rilpivirine. |
General Principles
ART has evolved steadily and at times briskly, resulting in new classes of medications to address emergent drug resistance, dosing convenience, coformulation capacity, reduced drug-drug interactions, and reduced toxic effects. Patients who have had persistent virologic suppression on older ART regimens that contained agents associated with long-term, organ-specific, or metabolic adverse effects; had food or fluid intake restrictions; or had dosing frequency and pill burden challenges may seek to have their regimens reviewed for opportunities to simplify or reduce the potential toxic effects of their current medications. Such switches may lead to improved adherence, enhanced quality of life, persistence in treatment, and reduced long-term adverse effects.
Regimen changes should be based on shared decision-making and not be driven by any hype surrounding around the newest regimen. It is appropriate for clinicians to discuss new treatment options with their patients as they become available so that they may benefit from an unbiased evaluation. Sometimes the issue of an ART regimen switch is raised because of insurance coverage restrictions or a patient’s out-of-pocket expenses. As with consideration of any ART switch, decisions in must be guided by the principles of enhancing efficacy, safety, and durability of therapeutic response.
All ART changes should be planned carefully because regimen failure after the switch is always possible. The goal of the regimen change should be clearly defined and the new regimen assessed for potential adverse effects due to unrecognized preexisting drug resistance, effect on chronic comorbid conditions (e.g., hepatitis B virus [HBV] infection, cardiovascular disease, obesity), and exposure to other chronic concurrent medications, especially when switching to or from an antiretroviral medication that is an inducer, inhibitor, or substrate of cytochrome P450 3A or P-glycoprotein.
Switching to a 3-Drug Single-Tablet Regimen
Studies in which a switch from a multi-tablet ART regimen to a 3-drug single-tablet regimen was made for simplification in participants with effective viral suppression are discussed below. Many of these trials were developed and conducted by pharmaceutical companies. Results must be interpreted with care because they may be biased as a result of numerous factors, including open-label study design and recruitment of participants dissatisfied with their ART regimen or looking for new options or participants with a proven record of adherence (i.e., virally suppressed at trial entry).
Integrase strand transfer inhibitor (INSTI)-based switches: Including switches to tenofovir alafenamide/emtricitabine/ bictegravir (TAF/FTC/BIC) and INSTI-to-INSTI within-class switches:
- Switch for safety and tolerability: Gilead Study 380-1844, a double-blind study designed to explore options to avoid abacavir (ABC)-associated cardiovascular concerns or dolutegravir (DTG)-associated neuropsychiatric concerns, randomly assigned 563 adults who were virally suppressed on a regimen of abacavir/lamivudine/dolutegravir (ABC/3TC/DTG) 1:1 to remain on their current therapy or switch to TAF/FTC/BIC Molina, et al. 2018. The study found TAF/FTC/BIC to be noninferior to remaining on ABC/3TC/DTG based on viral load suppression at week 48. No resistance emerged in either arm. No difference was found in adverse effects except for more gastrointestinal-related complaints among participants in the DTG arm.
- Switch from a boosted protease inhibitor (PI)-based regimen to TAF/FTC/BIC: Gilead Study 380-1878 was an open-label phase 3 study that enrolled 577 virologically suppressed adults taking a nucleoside/nucleotide reverse transcriptase inhibitor (NRTI; tenofovir disoproxil fumarate [TDF]- or ABC-based) plus a boosted PI (ritonavir [RTV] or cobicistat [COBI] with darunavir [DRV] or atazanavir [ATV]) who were randomized to remain on their baseline therapy or switch to TAF/FTC/BIC Daar, et al. 2018. At 48 weeks, the switch was noninferior with regard to viral suppression (HIV RNA <50 copies/mL), and the regimens in both arms were well tolerated. More treatment-related adverse effects occurred in the TAF/FTC/BIC group, especially headache, with most being mild or moderate in intensity. Discontinuation due to adverse effects was 1% or less in both arms. At week 96, viral suppression on a TAF/FTC/BIC regimen was maintained after the switch despite blips or baseline resistance-associated mutations (RAMs) Sax, et al. 2022.
- Switch to an INSTI-based single-tablet regimen (ABC/3TC/DTG): In the open-label STRIIVING study, 553 virally suppressed adults who were HLA-B*5701 negative with no history of treatment failure on non-nucleoside reverse transcriptase inhibitor (NNRTI)-, PI-, or INSTI-based regimens were randomized 1:1 to switch immediately to ABC/3TC/DTG or continue their current therapy for 24 weeks, after which all participants received ABC/3TC/DTG Trottier, et al. 2017. Switching was noninferior to remaining on current therapy with regard to viral suppression. Although more participants reported adverse effects in the switch arm at 48 weeks (75% vs. 60%), most were mild or moderate, and 4% of participants discontinued treatment because of adverse effects.
- Switch to a 3-drug NNRTI-based single-tablet regimen (TDF/3TC/doravirine [DOR]): DRIVE-SHIFT was an open-label study of 670 adults with HIV viral suppression on an NNRTI-, INSTI-, or PI-based regimen randomized 2:1 to switch to TDF/3TC/DOR or remain on current therapy Johnson, et al. 2019. At 48 weeks, viral suppression data demonstrated that TDF/3TC/DOR was noninferior to continuing the baseline regimen. TDF/3TC/DOR was well tolerated, leading to treatment discontinuation in 2.5% of participants. Long-term viral suppression was sustained through week 144 Kumar, et al. 2021.
- Switch to a 3-drug NNRTI-based single-tablet regimen (TAF/FTC/rilpivirine [RPV]): Two randomized, double‐blind, active‐controlled, noninferiority trials in adults with HIV taking TDF/FTC/RPV (Study 1216; N = 630) or TDF/FTC/efavirenz (Study 1160; N = 875) reported noninferior viral suppression at 96 weeks following 1:1 randomization in each to switch to TAF/FTC/RPV or remain on current therapy Hagins, et al. 2018; DeJesus, et al. 2017. Improvement in renal and bone parameters was noted among the participants who switched to TAF/FTC/RPV Hagins, et al. 2018; DeJesus, et al. 2017.
- Switch to a boosted PI-based single-tablet regimen (TAF/FTC/DRV/COBI): The EMERALD study, which included 1,141 virally suppressed adults who may have experienced previous non-DRV treatment failure, randomized participants 2:1 to switch to TAF/FTC/DRV/COBI or to remain on their current regimen for 48 weeks, with a late-switch additional extension phase (N = 1,080) through week 96. TAF/FTC/DRV/COBI effectively maintained viral suppression (no comparator for the extension phase). Furthermore, the study demonstrated the high genetic barrier of the regimen in that no primary PI, tenofovir, or FTC RAMs emerged during treatment and no participants withdrew because of lack of efficacy; 2% withdrew for adverse effects, renal and bone parameters were improved from baseline, and a small increase in total cholesterol to high-density lipoprotein cholesterol ratio was observed Eron, et al. 2019.
Switching to a 2-Drug Single-Tablet Regimen
Studies in which a switch from a 3- or 4-drug ART regimen to a 2-drug single-tablet regimen was made for simplification in participants with effective viral suppression are discussed below.
Note: Currently available 2-drug single-tablet regimens are not effective for treatment of pregnant patients or those who have HIV/HBV coinfection.
- Switch from a 3- or 4-drug regimen to 2-drug NNRTI/INSTI regimen (RPV/DTG): SWORD 1 and 2 were identical multinational, open-label studies that included 1,024 virally suppressed adults taking standard 3- or 4-drug ART regimens who were randomized 1:1 to switch to RPV/DTG for 52 weeks, followed by a late switch (N = 477) through 100 weeks of follow-up. Viral suppression was noninferior in the early switch compared with the late-switch group, and the 2-drug regimen was well tolerated Aboud(b), et al. 2019; Llibre, et al. 2018.
- Switch from TAF-based 3- or 4-drug regimen to 2-drug NRTI/INSTI regimen (3TC/DTG):
- The TANGO study was an open-label, multicenter study of 741 virally suppressed adults taking a 3- or 4-drug TAF-containing ART regimen who were randomized 1:1 to switch to the 2-drug regimen of 3TC/DTG or continue current therapy for 48 weeks. The 2-drug regimen was noninferior in maintaining viral suppression, and breakthrough virus did not demonstrate emergent INSTI or 3TC RAMs. M184V/I mutations were found at baseline (by proviral DNA assay) in 4 of 322 participants randomized to the 3TC/DTG arm, all 4 of whom maintained viral suppression. In the 3TC/DTG arm, 3.5% withdrew because of adverse effects van Wyk, et al. 2020. Baseline proviral DNA genotypic testing samples were obtained from 89% of participants in the 3TC/DTG arm and 87% in the TAF-containing arm and subsequently analyzed to identify if archived resistance could affect outcome at week 48 van Wyk, et al. 2020. Major NRTI RAMs were identified in 8% (1% had M184V) of proviral DNA in the 3TC/DTG arm and 5% (<1% with M184V) in the TAF-containing arm, and major INSTI RAMs were identified in 3 participants (<1%) in the 3TC/DTG arm and 5 (1%) in the TAF-containing arm. In both arms, all participants with major NRTI or INSTI RAMs maintained 100% viral suppression at week 48.
- The ART-PRO study included 41 INSTI-naive, virally suppressed adults with (n = 21) and without (n = 20) a history of 3TC-resistant mutations but with a negative proviral DNA test result (Sanger and next-generation sequencing) at the time of enrollment. Investigators speculated that the preexisting mutations had decayed over the course of long-term viral suppression in participants who switched their suppressive 3- or 4-drug ART regimen to 3TC/DTG. The median time from identification of 3TC RAMs and DNA sequencing was 12.9 years. Following the switch, 4 of 21 participants with historical 3TC resistance and 6 of 20 without past 3TC resistance had transient viremia; all participants were resuppressed at 48 weeks, 3TC RAMs did not reemerge during the transient viremia, and no INSTI RAMs were detected De Miguel, et al. 2020.
- The SALSA study included 493 virally suppressed adults who were randomized 1:1 to maintain their 3-drug regimen (2 NRTIs plus an NNRTI, PI, or INSTI) or switch to 3TC/DTG. All participants had no documented NRTI or INSTI RAMs and no history of treatment failure Llibre, et al. 2022. Proviral DNA genotypic resistance test results obtained before randomization were available from 377 participants (192 from the 3TC/DTG arm and 185 from the 3-drug arm) and were reviewed for the presence of baseline RAMs on post hoc analysis. Major NRTI RAMs were found in 8% of the 3TC/DTG arm (including 3% with the 3TC RAM M184V) and 9% of the 3-drug arm (including 2% with M184V). Major INSTI RAMs were found in 1 participant (<1%) in the 3TC/DTG arm and 4 (2%) in the 3-drug arm. Suppression of HIV RNA to <40 copies/mL was maintained in 80% of participants (4 of 5) with M184V in the 3TC/DTG arm and 50% (2 of 4) in the 3-drug arm, and 100% (1 of 1) and 100% (4 of 4) of participants with major INSTI RAMs in the 3TC/DTG and 3-drug arms, respectively. This study supports the effectiveness of the 2-drug regimen of 3TC/DTG when a patient has low-level preexisting RAMs, but because of the small numbers involved, these data do not change the recommendation to avoid use if such resistance is known.
- A substudy of the phase 2a, open-label, single-arm, multicenter VOLVER study focused on the utility of proviral DNA testing to predict treatment failure after a switch to 3TC/DTG in 121 virologically suppressed participants without chronic HBV infection, with past confirmed (M184V/I or K65R RAMs) or suspected (2 or more consecutive HIV viral loads >200 copies/mL while on ART including FTC or 3TC) 3TC resistance, and no M184V/I or K65R mutations on screening with proviral DNA Sanger genotyping and no history of INSTI failure De Miguel Buckley, et al. 2024. Use of next-generation sequencing (NGS) of proviral DNA for the presence of M184V/I (5% threshold) did not predict maintenance of viral suppression. The median time from documented 3TC resistance detection was 15.2 years. Because these individuals were already prescreened with Sanger sequence genotyping (gold standard) for the presence of resistance, and the threshold for NGS was set at 5% (compared with the commercial assay at 10%), and the long period of suppression, the archive of 3TC-resistant virus may have been too low to be clinically significant in the presence of a fully active second-generation INSTI. Further study will be necessary to determine if 3TC/DTG could be reliably effective in virus with higher levels of archived M184V substitution.
- In the open-label SOLAR-3D study, 100 heavily treatment-experienced participants who were virally suppressed on multi-drug ART regimens, half of whom had a history of M184V/I mutations, the majority were on ABC/3TC/DTG, were switched to 3TC/DTG Blick, et al. 2024. Participants with virus containing M184V/I were older, on ART longer, had a lower CD4 cell count nadir, had taken more antiretroviral medications, and had been virally suppressed longer. By intention-to-treat analysis, after switch there was no difference in viral suppression rate (HIV RNA <50 copies/mL) at 144 weeks between participants with (74%) or without (72%) historical M184V/I mutations, with no emergent resistance in either arm. A literature review and meta-analysis of 5 randomized controlled trials and 5 real-world studies that included virally suppressed individuals with historical M184V/I mutations who were switched to 3TC/DTG identified virologic failure ranging from 0.0% to 3.76% over 96 weeks without emergence of INSTI RAMs Kabra, et al. 2022. These data assuage concerns that use of DTG/3TC in the presence of unrecognized M184V/I mutation might lead to high levels of treatment failure, but do not address the question of whether a regimen with 3 or different active drugs would be more effective for long-term viral suppression in this scenario.
- The PASO-DOBLE (GeSIDA 11720) study enrolled 553 participants who were taking suppressive multi-tablet (>1) ART regimens containing TDF, COBI, or EFV, had no known drug resistance, and were DTG and BIC naive, and randomized them 1:1 to switch to either 3TC/DTG or TAF/FTC/BIC Ryan, et al. 2024. The study endpoints focused on safety, efficacy, tolerability, and weight change at 48 weeks. 3TC/DTG was found to be noninferior to TAF/FTC/BIC (HIV RNA <50 copies/mL in 93.1% and 89.9%, respectively), with no emergence of drug resistance. Participants in the 3TC/DTG arm, especially those who switched from ABC- or TDF-containing regimens, gained less weight than those in the TAF/FTC/BIC arm (0.89 kg vs. 1.81 kg; P=.016).
Switching to 2-Drug Injectable Therapy
Note: Currently available 2-drug injectable therapies are not effective for treatment of pregnant individuals or those who have HIV/HBV coinfection.
2-drug injectable ART for patients with viral suppression: Phase 3 clinical trial results suggest that CAB/RPV LA may be a suitable option for patients on suppressive ART with no major INSTI or NNRTI (excluding K103N) RAMs on proviral DNA or historical RNA genotypic tests who would prefer an alternative to daily oral therapy Overton, et al. 2021; Orkin, et al. 2020; Rizzardini, et al. 2020; Swindells, et al. 2020.
| KEY POINT |
|
2-drug injectable ART for patients without viral suppression: An off-label, nonrandomized study examined CAB/RPV LA use among patients with medication adherence challenges in a single safety-net clinic Gandhi, et al. 2023. The study population had high rates of unstable housing, substance use, and mental illness, and many participants had an unsuppressed HIV viral load when initiating or switching to CAB/RPV LA. The study enrolled 133 people with HIV who initiated CAB/RPV LA over an 18-month period. Participants were not required to have viral suppression at entry, had to commit to return every 4 weeks for injections, and had no RPV or INSTI RAMs (last criteria added after 2 emergent treatment failures); 38% of participants were Latinx, 16% were Black, and 14% were multiracial. Additionally, 8% were homeless and 58% were unstably housed, 100% were on government insurance, 38% had major mental illness, 43% were not virally suppressed (HIV RNA >30 copies/mL; median log10 HIV RNA 4.21), and 74% received on-time injections. After the switch to CAB/RPV LA, all of the 57% (n=76) of participants with viral suppression at initiation maintained it, and 96% of participants (55 of 57) who were not virally suppressed at initiation achieved viral suppression. At 48 weeks, 93% of participants who were initially unsuppressed had HIV viral loads <50 copies/mL Hickey, et al. 2024. Within the first 24 weeks, 2 virologic failures with resistance occurred before baseline resistance criteria were strengthened Gandhi, et al. 2023. The overall treatment failure rate was 1.5%, similar to those reported in the ATLAS and FLAIR studies. Per-protocol injections were delivered every 4 weeks, with the option to transition to every 8 weeks if viral suppression was achieved and maintained for 3 to 6 months Hickey, et al. 2025. Individuals with previously unsuppressed virus transitioning to every-8-week dosing of CAB/RPV LA may benefit from enhanced reminder calls and closer adherence support. This study addresses the minority population of people with HIV who have not achieved viral suppression with oral therapy but are the majority of those diagnosed with viremic HIV. Of note, CAB/RPV LA use in this study was accompanied by extensive case management, incentivization ($10 grocery vouchers for every-4-week dosing), social support, and outreach services with access to mental health and substance use wraparound services. The success of CAB/RPV LA in this population in the absence of comprehensive support services is unknown.
The results above were replicated in a small case series of 12 patients in Mississippi, all of whom were Black or Native American and 58% of whom were cisgender women. Mean viral load was 152,657 copies/mL, mean CD4 count was 233 cells/mm3, 1 participant had a primary INSTI RAM (N155H), and all achieved viral suppression on CAB/RPV LA by month 3 with no viral rebound to >200 copies/mL on follow-up (1 to 17 months); 77 of 82 injection visits occurred within the dosing window Brock, et al. 2024. Similarly, in a study of 325 individuals with HIV initiating CAB/RPV LA in the New York City municipal health system, 17 with unsuppressed HIV (median baseline viral load of 21,045 copies/mL, range 390–152,997 copies/mL) achieved high rates of viral suppression (76% achieved viral load <200 copies/mL) despite a high prevalence of social barriers including housing instability, unemployment, financial needs, and lack of insurance Gerber, et al. 2025.
The phase 3, randomized, multicenter, open-label ACTG A5359 study (LATITUDE), which included 434 people with HIV prescribed ART for at least 6 months who had viral loads >200 copies/mL at 2 time points at least 4 weeks apart or poor retention in care (2 missed appointments in 6 months or gap in medication of >7 days), compared CAB/RPV LA with continued standard of care (SOC) oral therapy Rana, et al. 2024. Participants received up to 24 weeks of incentive payments to promote achievement of viral suppression. Those who achieved viral loads <200 copies/mL (n= 294) after 4 weeks were randomized 1:1 to CAB/RPV (oral lead in for 4 weeks followed by monthly intramuscular injection) or continued SOC for 52 weeks. The incentives were not continued after randomization. The primary endpoint of regimen failure occurred in 28 participants (24.1%) in the CAB/RPV LA arm and 47 (38.5%) in the SOC arm, and the study was stopped by the Data and Safety Monitoring Board (DSMB) based on the finding of superiority of the CAB/RPV LA arm. Adverse effects were similar in both arms. Future studies to determine the need for viral suppression before initiating CAB/RPV LA in individuals facing adherence challenges with oral ART may be difficult to perform given the DSMB’s assessment of the superiority of CAB/RPV LA in the LATITUDE study.
An off-label use of the 2-drug injectable combination of the capsid inhibitor lenacapavir (LEN) plus CAB with or without RPV has been described in a case series of 34 people with HIV who had challenges in maintaining adherence to oral ART Gandhi, et al. 2024. LEN was used with CAB/RPV in 68%, in individuals with INSTI-resistant virus, high body mass index, or high viral load. LEN was used with CAB alone in 32%, in individuals with documented or suspected NNRTI-resistant virus. At 8 weeks, HIV viral suppression <75 copies/mL had increased from 47% to 94% of participants. All participants with NNRTI-resistant virus were virally suppressed on LEN/CAB. The authors called for further investigation in a clinical trial. In a retrospective review, 75 of 81 (93%) highly treatment-experienced individuals with HIV with viremia (9 with perinatally acquired HIV) achieved viral suppression after 1 to 2 injections of CAB/RPV alone (n = 56), CAB/RPV plus LEN (n = 23), or CAB/RPV plus LEN plus ibalizumab (n = 2) despite high rates of social needs Colasanti, et al. 2025.
Modeling studies have shown that off-label use of long-acting injectable ART in the setting of unsuppressed viremia may be most beneficial to individuals with HIV who have low CD4 counts, especially those facing unremitting challenges to adherence, such as cognitive impairment, substance use, homelessness, mental illness, and lack of social support Chen, et al. 2023. Shared decision-making might include discussions focused on success, removing obstacles to treatment, and achievement of viral suppression rather than the burden of daily adherence to oral therapy.
Resumption of ART After a Treatment Interruption
| RECOMMENDATIONS |
Resumption of ART After a Treatment Interruption
|
If a patient with HIV has a period of ART interruption, several potential areas of concern must be assessed at the time of treatment reinitiation, including the circumstances or reason for the interruption, the level of the viral load at the time of the interruption, the length of the interruption, and the level of treatment adherence before the interruption.
The simplest scenario is a treatment interruption due to unforeseen circumstances, such as loss of medication, travel without access to medication, or a gap in insurance coverage, in which the viral load was undetectable at the time of the interruption and all ART medications were used without missed doses and stopped simultaneously. In this scenario, the emergence of resistance to antiretroviral medications is unlikely, and the previously suppressive ART regimen can be restarted as soon as it is available [Jülg and Goebel 2006]. An exception to this scenario is with use of a combination with a prolonged clearance rate (such as injectable rilpivirine/cabotegravir or oral efavirenz) in which 1 or more drugs may persist at low levels, allowing selective pressure for resistance-associated mutations (RAMs) to be present over an extended period Landovitz, et al. 2020.
If the pre-interruption viral load was not suppressed and the patient had been on their ART regimen for more than 6 months or had a prolonged period of intermittent adherence before completely stopping treatment, drug resistance may have emerged before the interruption. As previously discussed, if treatment interruption is <4 weeks, a standard genotype test is recommended to demonstrate emergent RAMs.
After ≥4 weeks, if no or incomplete genotypic resistance test results are available, a proviral DNA genotype test is recommended. If the viral load was not suppressed before treatment interruption, reinitiating treatment with a regimen with a low genetic resistance barrier (e.g., 2 nucleoside/nucleotide reverse transcriptase inhibitors [NRTIs] + a first-generation non-nucleoside reverse transcriptase inhibitor [NNRTI] or first-generation integrase strand transfer inhibitor [INSTI]) may be unsuccessful. Considering a regimen with a higher genetic resistance barrier (2 NRTIs + a second-generation INSTI or boosted protease inhibitor [PI]) or intensifying the regimen by adding a drug with a high genetic resistance barrier (a second-generation INSTI or boosted PI) would be appropriate. The regimen can be simplified once viral suppression is obtained and results of genotypic resistance testing are available.
All Recommendations
| ALL RECOMMENDATIONS: SECOND-LINE ART AFTER TREATMENT FAILURE OR FOR REGIMEN SIMPLIFICATION |
Identifying and Managing Virologic Failure
Changes to Address Drug Resistance
Changes to Address Adverse Effects
Changes to Address Drug-Drug Interactions
Changes Due to Pregnancy
Changes for Regimen Simplification
Resumption of ART After a Treatment Interruption
|
Abbreviations: 3TC, lamivudine; ART, antiretroviral therapy; ART, antiretroviral therapy; ARV, antiretroviral medication; BIC, bictegravir; CAB/RPV LA, long-acting cabotegravir and rilpivirine; COBI, cobicistat; DHHS, U.S. Department of Health and Human Services; DRV, darunavir; DTG, dolutegravir; ETV, entecavir; FTC, emtricitabine; HBV, hepatitis B virus; INSTI, integrase strand transfer inhibitor; PI, protease inhibitor; RAM, resistance-associated mutation; RTV, retonavir; TAF, tenofovir alafenamide; TDF, tenofovir disoproxil fumarate. |
Shared Decision-Making
Download Printable PDF of Shared Decision-Making Statement
Date of current publication: August 8, 2023
Lead authors: Jessica Rodrigues, MS; Jessica M. Atrio, MD, MSc; and Johanna L. Gribble, MA
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: August 8, 2023
Rationale
Throughout its guidelines, the New York State Department of Health (NYSDOH) AIDS Institute (AI) Clinical Guidelines Program recommends “shared decision-making,” an individualized process central to patient-centered care. With shared decision-making, clinicians and patients engage in meaningful dialogue to arrive at an informed, collaborative decision about a patient’s health, care, and treatment planning. The approach to shared decision-making described here applies to recommendations included in all program guidelines. The included elements are drawn from a comprehensive review of multiple sources and similar attempts to define shared decision-making, including the Institute of Medicine’s original description [Institute of Medicine 2001]. For more information, a variety of informative resources and suggested readings are included at the end of the discussion.
Benefits
The benefits to patients that have been associated with a shared decision-making approach include:
- Decreased anxiety [Niburski, et al. 2020; Stalnikowicz and Brezis 2020]
- Increased trust in clinicians [Acree, et al. 2020; Groot, et al. 2020; Stalnikowicz and Brezis 2020]
- Improved engagement in preventive care [McNulty, et al. 2022; Scalia, et al. 2022; Bertakis and Azari 2011]
- Improved treatment adherence, clinical outcomes, and satisfaction with care [Crawford, et al. 2021; Bertakis and Azari 2011; Robinson, et al. 2008]
- Increased knowledge, confidence, empowerment, and self-efficacy [Chen, et al. 2021; Coronado-Vázquez, et al. 2020; Niburski, et al. 2020]
Approach
Collaborative care: Shared decision-making is an approach to healthcare delivery that respects a patient’s autonomy in responding to a clinician’s recommendations and facilitates dynamic, personalized, and collaborative care. Through this process, a clinician engages a patient in an open and respectful dialogue to elicit the patient’s knowledge, experience, healthcare goals, daily routine, lifestyle, support system, cultural and personal identity, and attitudes toward behavior, treatment, and risk. With this information and the clinician’s clinical expertise, the patient and clinician can collaborate to identify, evaluate, and choose from among available healthcare options [Coulter and Collins 2011]. This process emphasizes the importance of a patient’s values, preferences, needs, social context, and lived experience in evaluating the known benefits, risks, and limitations of a clinician’s recommendations for screening, prevention, treatment, and follow-up. As a result, shared decision-making also respects a patient’s autonomy, agency, and capacity in defining and managing their healthcare goals. Building a clinician-patient relationship rooted in shared decision-making can help clinicians engage in productive discussions with patients whose decisions may not align with optimal health outcomes. Fostering open and honest dialogue to understand a patient’s motivations while suspending judgment to reduce harm and explore alternatives is particularly vital when a patient chooses to engage in practices that may exacerbate or complicate health conditions [Halperin, et al. 2007].
Options: Implicit in the shared decision-making process is the recognition that the “right” healthcare decisions are those made by informed patients and clinicians working toward patient-centered and defined healthcare goals. When multiple options are available, shared decision-making encourages thoughtful discussion of the potential benefits and potential harms of all options, which may include doing nothing or waiting. This approach also acknowledges that efficacy may not be the most important factor in a patient’s preferences and choices [Sewell, et al. 2021].
Clinician awareness: The collaborative process of shared decision-making is enhanced by a clinician’s ability to demonstrate empathic interest in the patient, avoid stigmatizing language, employ cultural humility, recognize systemic barriers to equitable outcomes, and practice strategies of self-awareness and mitigation against implicit personal biases [Parish, et al. 2019].
Caveats: It is important for clinicians to recognize and be sensitive to the inherent power and influence they maintain throughout their interactions with patients. A clinician’s identity and community affiliations may influence their ability to navigate the shared decision-making process and develop a therapeutic alliance with the patient and may affect the treatment plan [KFF 2023; Greenwood, et al. 2020]. Furthermore, institutional policy and regional legislation, such as requirements for parental consent for gender-affirming care for transgender people or insurance coverage for sexual health care, may infringe upon a patient’s ability to access preventive- or treatment-related care [Sewell, et al. 2021].
Figure 1: Elements of Shared Decision-Making
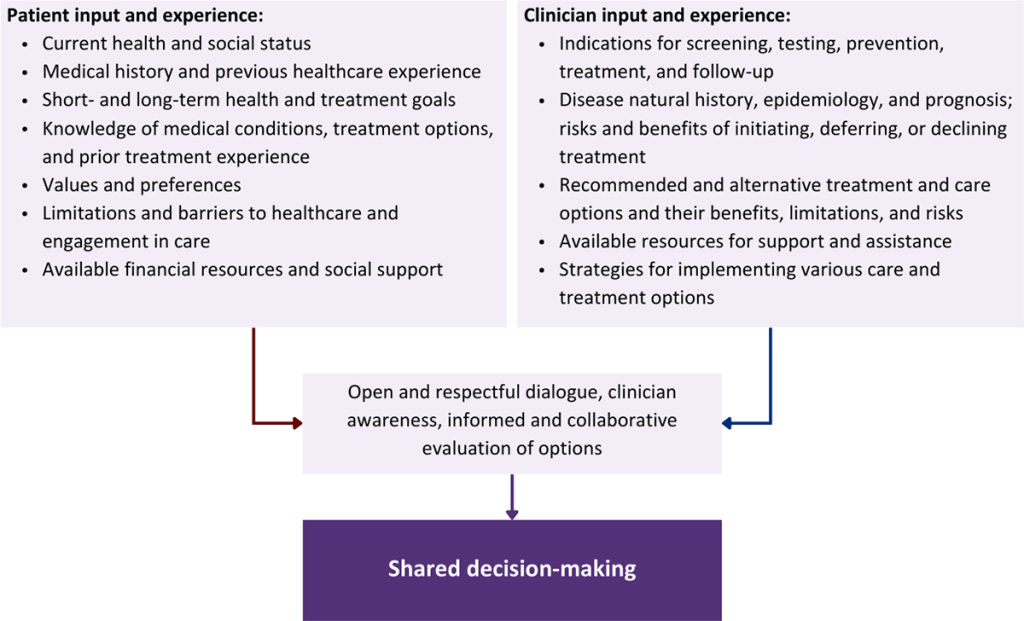
Health equity: Adapting a shared decision-making approach that supports diverse populations is necessary to achieve more equitable and inclusive health outcomes [Castaneda-Guarderas, et al. 2016]. For instance, clinicians may need to incorporate cultural- and community-specific considerations into discussions with women, gender-diverse individuals, and young people concerning their sexual behaviors, fertility intentions, and pregnancy or lactation status. Shared decision-making offers an opportunity to build trust among marginalized and disenfranchised communities by validating their symptoms, values, and lived experience. Furthermore, it can allow for improved consistency in patient screening and assessment of prevention options and treatment plans, which can reduce the influence of social constructs and implicit bias [Castaneda-Guarderas, et al. 2016].
Clinician bias has been associated with health disparities and can have profoundly negative effects [FitzGerald and Hurst 2017; Hall, et al. 2015]. It is often challenging for clinicians to recognize and set aside personal biases and to address biases with peers and colleagues. Consciously or unconsciously, negative or stigmatizing assumptions are often made about patient characteristics, such as race, ethnicity, gender, sexual orientation, mental health, and substance use [Avery, et al. 2019; van Boekel, et al. 2013; Livingston, et al. 2012]. With its emphasis on eliciting patient information, a shared decision-making approach encourages clinicians to inquire about patients’ lived experiences rather than making assumptions and to recognize the influence of that experience in healthcare decision-making.
Stigma: Stigma may prevent individuals from seeking or receiving treatment and harm reduction services [Tsai, et al. 2019]. Among people with HIV, stigma and medical mistrust remain significant barriers to healthcare utilization, HIV diagnosis, and medication adherence and can affect disease outcomes [Turan, et al. 2017; Chambers, et al. 2015], and stigma among clinicians against people who use substances has been well-documented [Stone, et al. 2021; Tsai, et al. 2019; van Boekel, et al. 2013]. Sexual and reproductive health, including strategies to prevent HIV transmission, acquisition, and progression, may be subject to stigma, bias, social influence, and violence.
| SHARED DECISION-MAKING IN HIV CARE |
|
Resources and Suggested Reading
In addition to the references cited below, the following resources and suggested reading may be useful to clinicians.
| RESOURCES |
References
Acree ME, McNulty M, Blocker O, et al. Shared decision-making around anal cancer screening among black bisexual and gay men in the USA. Cult Health Sex 2020;22(2):201-16. [PMID: 30931831]
Avery JD, Taylor KE, Kast KA, et al. Attitudes toward individuals with mental illness and substance use disorders among resident physicians. Prim Care Companion CNS Disord 2019;21(1):18m02382. [PMID: 30620451]
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med 2011;24(3):229-39. [PMID: 21551394]
Castaneda-Guarderas A, Glassberg J, Grudzen CR, et al. Shared decision making with vulnerable populations in the emergency department. Acad Emerg Med 2016;23(12):1410-16. [PMID: 27860022]
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health 2015;15:848. [PMID: 26334626]
Chen CH, Kang YN, Chiu PY, et al. Effectiveness of shared decision-making intervention in patients with lumbar degenerative diseases: a randomized controlled trial. Patient Educ Couns 2021;104(10):2498-2504. [PMID: 33741234]
Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, et al. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore) 2020;99(32):e21389. [PMID: 32769870]
Coulter A, Collins A. Making shared decision-making a reality: no decision about me, without me. 2011. https://www.kingsfund.org.uk/sites/default/files/Making-shared-decision-making-a-reality-paper-Angela-Coulter-Alf-Collins-July-2011_0.pdf
Crawford J, Petrie K, Harvey SB. Shared decision-making and the implementation of treatment recommendations for depression. Patient Educ Couns 2021;104(8):2119-21. [PMID: 33563500]
FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics 2017;18(1):19. [PMID: 28249596]
Greenwood BN, Hardeman RR, Huang L, et al. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020;117(35):21194-21200. [PMID: 32817561]
Groot G, Waldron T, Barreno L, et al. Trust and world view in shared decision making with indigenous patients: a realist synthesis. J Eval Clin Pract 2020;26(2):503-14. [PMID: 31750600]
Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health 2015;105(12):e60-76. [PMID: 26469668]
Halperin B, Melnychuk R, Downie J, et al. When is it permissible to dismiss a family who refuses vaccines? Legal, ethical and public health perspectives. Paediatr Child Health 2007;12(10):843-45. [PMID: 19043497]
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. 2001. https://www.ncbi.nlm.nih.gov/books/NBK222274/
KFF. Key data on health and health care by race and ethnicity. 2023 Mar 15. https://www.kff.org/racial-equity-and-health-policy/report/key-data-on-health-and-health-care-by-race-and-ethnicity/ [accessed 2023 May 19]
Livingston JD, Milne T, Fang ML, et al. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction 2012;107(1):39-50. [PMID: 21815959]
McNulty MC, Acree ME, Kerman J, et al. Shared decision making for HIV pre-exposure prophylaxis (PrEP) with black transgender women. Cult Health Sex 2022;24(8):1033-46. [PMID: 33983866]
Niburski K, Guadagno E, Abbasgholizadeh-Rahimi S, et al. Shared decision making in surgery: a meta-analysis of existing literature. Patient 2020;13(6):667-81. [PMID: 32880820]
Parish SJ, Hahn SR, Goldstein SW, et al. The International Society for the Study of Women’s Sexual Health process of care for the identification of sexual concerns and problems in women. Mayo Clin Proc 2019;94(5):842-56. [PMID: 30954288]
Robinson JH, Callister LC, Berry JA, et al. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008;20(12):600-607. [PMID: 19120591]
Scalia P, Durand MA, Elwyn G. Shared decision-making interventions: an overview and a meta-analysis of their impact on vaccine uptake. J Intern Med 2022;291(4):408-25. [PMID: 34700363]
Sewell WC, Solleveld P, Seidman D, et al. Patient-led decision-making for HIV preexposure prophylaxis. Curr HIV/AIDS Rep 2021;18(1):48-56. [PMID: 33417201]
Stalnikowicz R, Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract 2020;26(2):431-38. [PMID: 31989727]
Stone EM, Kennedy-Hendricks A, Barry CL, et al. The role of stigma in U.S. primary care physicians’ treatment of opioid use disorder. Drug Alcohol Depend 2021;221:108627. [PMID: 33621805]
Tsai AC, Kiang MV, Barnett ML, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med 2019;16(11):e1002969. [PMID: 31770387]
Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav 2017;21(1):283-91. [PMID: 27272742]
van Boekel LC, Brouwers EP, van Weeghel J, et al. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013;131(1-2):23-35. [PMID: 23490450]
References
Aboud(a) M., Kaplan R., Lombaard J., et al. Dolutegravir versus ritonavir-boosted lopinavir both with dual nucleoside reverse transcriptase inhibitor therapy in adults with HIV-1 infection in whom first-line therapy has failed (DAWNING): an open-label, non-inferiority, phase 3b trial. Lancet Infect Dis 2019;19(3):253-64. [PMID: 30732940]
Aboud(b) M., Orkin C., Podzamczer D., et al. Efficacy and safety of dolutegravir-rilpivirine for maintenance of virological suppression in adults with HIV-1: 100-week data from the randomised, open-label, phase 3 SWORD-1 and SWORD-2 studies. Lancet HIV 2019;6(9):e576-87. [PMID: 31307948]
Abrams D., Lévy Y., Losso M. H., et al. Interleukin-2 therapy in patients with HIV infection. N Engl J Med 2009;361(16):1548-59. [PMID: 19828532]
AIDSmap. Food requirements for anti-HIV medications. 2023 Apr. https://www.aidsmap.com/about-hiv/food-requirements-anti-hiv-medications [accessed 2025 May 6]
Anderson D., Ramgopal M., Hagins D. P., et al. DEFINE: a prospective, randomized, phase 4 trial to assess a protease inhibitor-based regimen switch strategy to manage integrase inhibitor-related weight gain. Clin Infect Dis 2024. [PMID: 39230668]
Anderson J. A., Jiang H., Ding X., et al. Genotypic susceptibility scores and HIV type 1 RNA responses in treatment-experienced subjects with HIV type 1 infection. AIDS Res Hum Retroviruses 2008;24(5):685-94. [PMID: 18462083]
Andre-Garnier E., Bocket L., Bourlet T., et al. Use of genotypic HIV DNA testing: a DELPHI-type consensus. J Antimicrob Chemother 2024;79(3):578-88. [PMID: 38269616]
Andreatta K., D’Antoni M. L., Chang S., et al. Preexisting resistance and week 48 virologic outcomes after switching to B/F/TAF in African American adults with HIV. Open Forum Infect Dis 2020;7(Suppl 1):s183-84. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7777761/
Anstett K., Brenner B., Mesplede T., et al. HIV drug resistance against strand transfer integrase inhibitors. Retrovirology 2017;14(1):36. [PMID: 28583191]
APR. Antiretroviral Pregnancy Registry interim report for 1 January 1989 - 31 January 2024. 2024 Jul 1. https://apregistry.com/InterimReport.aspx [accessed 2025 May 6]
Bajema K. L., Nance R. M., Delaney J. A., et al. Substantial decline in heavily treated therapy-experienced persons with HIV with limited antiretroviral treatment options. AIDS 2020;34(14):2051-59. [PMID: 33055569]
Beccari M. V., Mogle B. T., Sidman E. F., et al. Ibalizumab, a novel monoclonal antibody for the management of multidrug-resistant HIV-1 infection. Antimicrob Agents Chemother 2019;63(6):e00110-19. [PMID: 30885900]
Benson C., Wang X., Dunn K. J., et al. Antiretroviral adherence, drug resistance, and the impact of social determinants of health in HIV-1 patients in the US. AIDS Behav 2020;24(12):3562-73. [PMID: 32488554]
Bernal E., Gómez J. M., Jarrín I., et al. Low-level viremia is associated with clinical progression in HIV-infected patients receiving antiretroviral treatment. J Acquir Immune Defic Syndr 2018;78(3):329-37. [PMID: 29543636]
Bi X., Gatanaga H., Ida S., et al. Emergence of protease inhibitor resistance-associated mutations in plasma HIV-1 precedes that in proviruses of peripheral blood mononuclear cells by more than a year. J Acquir Immune Defic Syndr 2003;34(1):1-6. [PMID: 14501787]
Blick G., Cerreta-Dial E., Mancini G., et al. No confirmed virological failures (CVF) for 144 weeks when switching 2-/3-/4-drug ART to DTG/3TC in heavily treatment-experienced PLWHA with prior M184V/I and virological failures (VF) in the prospective SOLAR-3D study. Abstract SS0403LB. 25th International AIDS Conference; 2024 Jul 22-26; Munich, Germany. https://doi.org/10.1002/jia2.26279
Bordes C., Leguelinel-Blache G., Lavigne J. P., et al. Interactions between antiretroviral therapy and complementary and alternative medicine: a narrative review. Clin Microbiol Infect 2020;26(9):1161-70. [PMID: 32360208]
Braun H. M., Candelario J., Hanlon C. L., et al. Transgender women living with HIV frequently take antiretroviral therapy and/or feminizing hormone therapy differently than prescribed due to drug-drug interaction concerns. LGBT Health 2017;4(5):371-75. [PMID: 28876170]
Brenner B. G., Coutsinos D. The K65R mutation in HIV-1 reverse transcriptase: genetic barriers, resistance profile and clinical implications. HIV Ther 2009;3(6):583-94. [PMID: 20190870]
Brock J. B., Herrington P., Hickman M., et al. Long-acting injectable cabotegravir/rilpivirine effective in a small patient cohort with virologic failure on oral antiretroviral therapy. Clin Infect Dis 2024;78(1):122-24. [PMID: 37740255]
Bruner K. M., Murray A. J., Pollack R. A., et al. Defective proviruses rapidly accumulate during acute HIV-1 infection. Nat Med 2016;22(9):1043-49. [PMID: 27500724]
Buckheit R. W. Understanding HIV resistance, fitness, replication capacity and compensation: targeting viral fitness as a therapeutic strategy. Expert Opin Investig Drugs 2004;13(8):933-58. [PMID: 15268633]
Cahn P., Fourie J., Grinsztejn B., et al. Week 48 analysis of once-daily vs. twice-daily darunavir/ritonavir in treatment-experienced HIV-1-infected patients. AIDS 2011;25(7):929-39. [PMID: 21346512]
Cahn P., Pozniak A. L., Mingrone H., et al. Dolutegravir versus raltegravir in antiretroviral-experienced, integrase-inhibitor-naive adults with HIV: week 48 results from the randomised, double-blind, non-inferiority SAILING study. Lancet 2013;382(9893):700-708. [PMID: 23830355]
Carnes S. K., Sheehan J. H., Aiken C. Inhibitors of the HIV-1 capsid, a target of opportunity. Curr Opin HIV AIDS 2018;13(4):359-65. [PMID: 29782334]
Castagna A., Maggiolo F., Penco G., et al. Dolutegravir in antiretroviral-experienced patients with raltegravir- and/or elvitegravir-resistant HIV-1: 24-week results of the phase III VIKING-3 study. J Infect Dis 2014;210(3):354-62. [PMID: 24446523]
Chahine E. B., Durham S. H. Ibalizumab: the first monoclonal antibody for the treatment of HIV-1 infection. Ann Pharmacother 2021;55(2):230-39. [PMID: 32659101]
Chen W., Gandhi M., Sax P. E., et al. Projected benefits of long-acting antiretroviral therapy in nonsuppressed people with human immunodeficiency virus experiencing adherence barriers. Open Forum Infect Dis 2023;10(8):ofad390. [PMID: 37601728]
Chu C., Armenia D., Walworth C., et al. Genotypic resistance testing of HIV-1 DNA in peripheral blood mononuclear cells. Clin Microbiol Rev 2022;35(4):e0005222. [PMID: 36102816]
Ciaffi L., Koulla-Shiro S., Sawadogo A. B., et al. Boosted protease inhibitor monotherapy versus boosted protease inhibitor plus lamivudine dual therapy as second-line maintenance treatment for HIV-1-infected patients in sub-Saharan Africa (ANRS12 286/MOBIDIP): a multicentre, randomised, parallel, open-label, superiority trial. Lancet HIV 2017;4(9):e384-92. [PMID: 28566227]
Cimino C., Binkley A., Swisher R., et al. Antiretroviral considerations in HIV-infected patients undergoing bariatric surgery. J Clin Pharm Ther 2018;43(6):757-67. [PMID: 30110123]
Clemente T., Reali P., Lolatto R., et al. Is it effective to switch regimen in PWH with low-level viremia in the current era? Abstract 671. CROI; 2025 Mar 9-12; San Francisco, CA. https://www.croiconference.org/abstract/3248-2025/
Cluck D. B., Chastain D. B., Murray M., et al. Consensus recommendations for the use of novel antiretrovirals in persons with HIV who are heavily treatment-experienced and/or have multidrug-resistant HIV-1: endorsed by the American Academy of HIV Medicine, American College of Clinical Pharmacy. Pharmacotherapy 2024;44(5):360-82. [PMID: 38853601]
Cohen C. J., Meyers J. L., Davis K. L. Association between daily antiretroviral pill burden and treatment adherence, hospitalisation risk, and other healthcare utilisation and costs in a US Medicaid population with HIV. BMJ Open 2013;3(8). [PMID: 23906955]
Colasanti J., Aldredge A., Niles Carnes L., et al. Long-acting injectable art in persons with HIV-1 viremia in the South: a tool to end the epidemic. Abstract 690. CROI; 2025 Mar 9-12; San Francisco, CA. https://www.croiconference.org/abstract/3829-2025/
Crespo-Bermejo C., de Arellano E. R., Lara-Aguilar V., et al. Persistent low-Level viremia in persons living with HIV undertreatment: an unresolved status. Virulence 2021;12(1):2919-31. [PMID: 34874239]
Curanovic D., Martens S. K., Rodriguez M. A., et al. HIV-1 DNA testing in viremic patients identifies more drug resistance than HIV-1 RNA testing. Open Forum Infect Dis 2023;10(4):ofad146. [PMID: 37065991]
Cutrell A. G., Schapiro J. M., Perno C. F., et al. Exploring predictors of HIV-1 virologic failure to long-acting cabotegravir and rilpivirine: a multivariable analysis. AIDS 2021;35(9):1333-42. [PMID: 33730748]
D'Antoni M. L., Andreatta K., Chang S., et al. Longitudinal analysis of preexisting resistance-associated mutations prior to B/F/TAF switch. Abstract 695. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/longitudinal-analysis-of-preexisting-resistance-associated-mutations-prior-to-b-f-taf-switch/
Daar E. S., DeJesus E., Ruane P., et al. Efficacy and safety of switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from boosted protease inhibitor-based regimens in virologically suppressed adults with HIV-1: 48 week results of a randomised, open-label, multicentre, phase 3, non-inferiority trial. Lancet HIV 2018;5(7):e347-56. [PMID: 29925490]
Daar E. S., Tierney C., Fischl M. A., et al. Atazanavir plus ritonavir or efavirenz as part of a 3-drug regimen for initial treatment of HIV-1. Ann Intern Med 2011;154(7):445-56. [PMID: 21320923]
Davy-Mendez T., Eron J. J., Brunet L., et al. New antiretroviral agent use affects prevalence of HIV drug resistance in clinical care populations. AIDS 2018;32(17):2593-2603. [PMID: 30134298]
de Meyer S., Azijn H., Surleraux D., et al. TMC114, a novel human immunodeficiency virus type 1 protease inhibitor active against protease inhibitor-resistant viruses, including a broad range of clinical isolates. Antimicrob Agents Chemother 2005;49(6):2314-21. [PMID: 15917527]
de Meyer S., Vangeneugden T., van Baelen B., et al. Resistance profile of darunavir: combined 24-week results from the POWER trials. AIDS Res Hum Retroviruses 2008;24(3):379-88. [PMID: 18327986]
De Miguel Buckley R., Sigcha M., de Lagarde M., et al. Impact of archived minority populations with M184V/I on DTG/3TC for maintenance of viral suppression. Abstract 693. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/impact-of-archived-minority-populations-with-m184v-i-on-dtg-3tc-for-maintenance-of-viral-suppression/
De Miguel R., Rial-Crestelo D., Dominguez-Dominguez L., et al. Dolutegravir plus lamivudine for maintenance of HIV viral suppression in adults with and without historical resistance to lamivudine: 48-week results of a non-randomized, pilot clinical trial (ART-PRO). EBioMedicine 2020;55:102779. [PMID: 32408111]
DeJesus E., McGary C. S., Mesquita P., et al. Comparable efficacy of ibalizumab in combination with 1 or 2 fully active agents. Abstract 507. CROI; 2020 Mar 8-11; Boston, MA. https://www.croiconference.org/abstract/comparable-efficacy-of-ibalizumab-in-combination-with-1-or-2-fully-active-agents/
DeJesus E., Ramgopal M., Crofoot G., et al. Switching from efavirenz, emtricitabine, and tenofovir disoproxil fumarate to tenofovir alafenamide coformulated with rilpivirine and emtricitabine in virally suppressed adults with HIV-1 infection: a randomised, double-blind, multicentre, phase 3b, non-inferiority study. Lancet HIV 2017;4(5):e205-13. [PMID: 28259776]
Delaugerre C., Gallien S., Flandre P., et al. Impact of low-level-viremia on HIV-1 drug-resistance evolution among antiretroviral treated-patients. PLoS One 2012;7(5):e36673. [PMID: 22590588]
Demirdjian S., Naik V., Margot N., et al. Phenotypic characterization of replication-impaired lenacapavir-resistant HIV clinical isolates. Abstract 681. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/phenotypic-characterization-of-replication-impaired-lenacapavir-resistant-hiv-clinical-isolates/
Derache A., Shin H. S., Balamane M., et al. HIV drug resistance mutations in proviral DNA from a community treatment program. PLoS One 2015;10(1):e0117430. [PMID: 25635815]
DHHS. Recommendations for the use of antiretroviral drugs during pregnancy and interventions to reduce perinatal HIV transmission in the United States. 2024 Dec 19. https://clinicalinfo.hiv.gov/en/guidelines/perinatal/whats-new-guidelines [accessed 2025 May 6]
Dinoso J. B., Kim S. Y., Wiegand A. M., et al. Treatment intensification does not reduce residual HIV-1 viremia in patients on highly active antiretroviral therapy. Proc Natl Acad Sci U S A 2009;106(23):9403-8. [PMID: 19470482]
Dorjee K., Choden T., Baxi S. M., et al. Risk of cardiovascular disease associated with exposure to abacavir among individuals with HIV: a systematic review and meta-analyses of results from 17 epidemiologic studies. Int J Antimicrob Agents 2018;52(5):541-53. [PMID: 30040992]
Dû D. le, Marigot-Outtandy D., Mathez D., et al. Maraviroc intensification in HIV-1 infected patients with persistant low-level viremia. J AIDS Clin Res 2016;7(6):578. https://doi.org/10.4172/2155-6113.1000578
Ebers A. M., Alkabab Y., Wispelwey B., et al. Efficacy of raltegravir, etravirine and darunavir/ritonavir for treatment-experienced HIV patients from a non-urban clinic population in the United States. Ther Adv Infect Dis 2017;4(5):135-42. [PMID: 28959444]
Ellis K. E., Nawas G. T., Chan C., et al. Clinical outcomes following the use of archived proviral HIV-1 DNA genotype to guide antiretroviral therapy adjustment. Open Forum Infect Dis 2020;7(1):ofz533. [PMID: 31915714]
Elvstam O., Marrone G., Medstrand P., et al. All-cause mortality and serious non-AIDS events in adults with low-level human immunodeficiency virus viremia during combination antiretroviral therapy: results from a Swedish nationwide observational study. Clin Infect Dis 2021;72(12):2079-86. [PMID: 32271361]
Elvstam O., Medstrand P., Yilmaz A., et al. Virological failure and all-cause mortality in HIV-positive adults with low-level viremia during antiretroviral treatment. PLoS One 2017;12(7):e0180761. [PMID: 28683128]
Emu B., Fessel J., Schrader S., et al. Phase 3 study of ibalizumab for multidrug-resistant HIV-1. N Engl J Med 2018;379(7):645-54. [PMID: 30110589]
Enriquez M., Cheng A. L., McKinsey D., et al. Peers keep it real: re-engaging adults in HIV care. J Int Assoc Provid AIDS Care 2019;18:2325958219838858. [PMID: 30950300]
Eron J. J., Cooper D. A., Steigbigel R. T., et al. Efficacy and safety of raltegravir for treatment of HIV for 5 years in the BENCHMRK studies: final results of two randomised, placebo-controlled trials. Lancet Infect Dis 2013;13(7):587-96. [PMID: 23664333]
Eron J. J., Orkin C., Cunningham D., et al. Week 96 efficacy and safety results of the phase 3, randomized EMERALD trial to evaluate switching from boosted-protease inhibitors plus emtricitabine/tenofovir disoproxil fumarate regimens to the once daily, single-tablet regimen of darunavir/cobicistat/emtricitabine/tenofovir alafenamide (D/C/F/TAF) in treatment-experienced, virologically-suppressed adults living with HIV-1. Antiviral Res 2019;170:104543. [PMID: 31279073]
Eron J. J., Young B., Cooper D. A., et al. Switch to a raltegravir-based regimen versus continuation of a lopinavir-ritonavir-based regimen in stable HIV-infected patients with suppressed viraemia (SWITCHMRK 1 and 2): two multicentre, double-blind, randomised controlled trials. Lancet 2010;375(9712):396-407. [PMID: 20074791]
Fagard C., Colin C., Charpentier C., et al. Long-term efficacy and safety of raltegravir, etravirine, and darunavir/ritonavir in treatment-experienced patients: week 96 results from the ANRS 139 TRIO trial. J Acquir Immune Defic Syndr 2012;59(5):489-93. [PMID: 22293546]
FDA. Sunlenca (lenacapavir) tablets, for oral use. 2024 Nov. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215973s006,215974s008lbl.pdf [accessed 2025 May 6]
Feder(a) A. F., Pennings P. S., Petrov D. A. The clarifying role of time series data in the population genetics of HIV. PLoS Genet 2021;17(1):e1009050. [PMID: 33444376]
Feder(b) A. F., Harper K. N., Brumme C. J., et al. Understanding patterns of HIV multi-drug resistance through models of temporal and spatial drug heterogeneity. Elife 2021;10:e69032. [PMID: 34473060]
Feng J., Sykes D., Peters P., et al. Transmitted drug resistance in people living with diagnosed HIV in California. CROI; 2020 Mar 8-11; Boston, MA. https://www.croiconference.org/abstract/transmitted-drug-resistance-in-people-living-with-diagnosed-hiv-in-california/
Ferretti F., Mackie N. E., Singh G. K. J., et al. Characterization of low level viraemia in HIV-infected patients receiving boosted protease inhibitor-based antiretroviral regimens. HIV Res Clin Pract 2019;20(4-5):107-10. [PMID: 32000615]
Fichtenbaum C. J., Malvestutto C. D., Watanabe M.G. Abacavir is associated with elevated risk for cardiovascular events in the REPRIEVE trial. Abstract OAB3406LB. 25th International AIDS Conference; 2024 Jul 22-26; Munich, Germany. https://www.natap.org/2024/IAS/IAS_19.htm
Fleming J., Mathews W. C., Rutstein R. M., et al. Low-level viremia and virologic failure in persons with HIV infection treated with antiretroviral therapy. AIDS 2019;33(13):2005-12. [PMID: 31306175]
Galizzi N., Galli L., Poli A., et al. Glomerular filtration rate estimated by cystatin C formulas in HIV-1 patients treated with dolutegravir, rilpivirine or cobicistat. New Microbiol 2018;41(4):256-61. [PMID: 30252923]
Gandhi M., Hill L., Grochowski J., et al. Case series examining the long-acting combination of lenacapavir and cabotegravir: call for a trial. Abstract 629. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/case-series-examining-the-long-acting-combination-of-lenacapavir-and-cabotegravir-call-for-a-trial/
Gandhi M., Salazar J., Hickey M.D., et al. High virologic suppression rates on long-acting art in a safety-net clinic population. Abstract 518. CROI; 2023 Feb 19-22; Seattle, WA. https://www.croiconference.org/abstract/high-virologic-suppression-rates-on-long-acting-art-in-a-safety-net-clinic-population/
Gandhi R. T., Tashima K. T., Smeaton L. M., et al. Long-term outcomes in a large randomized trial of HIV-1 salvage therapy: 96-week results of AIDS Clinical Trials Group A5241 (OPTIONS). J Infect Dis 2020;221(9):1407-1415. [PMID: 31135883]
Gandhi R. T., Zheng L., Bosch R. J., et al. The effect of raltegravir intensification on low-level residual viremia in HIV-infected patients on antiretroviral therapy: a randomized controlled trial. PLoS Med 2010;7(8). [PMID: 20711481]
Gatell J. M., Assoumou L., Moyle G., et al. Immediate versus deferred switching from a boosted protease inhibitor-based regimen to a dolutegravir-based regimen in virologically suppressed patients with high cardiovascular risk or age ≥50 years: final 96-week results of the NEAT022 study. Clin Infect Dis 2019;68(4):597-606. [PMID: 29912307]
Gerber A., Casey E., Mgbako O., et al. Outcomes of LAI ART for people with detectable HIV viremia in the NYC public healthcare system. Abstract 682. CROI; 2025 Mar 9-12; San Francisco, CA. https://www.croiconference.org/abstract/2881-2025/
Gilbert E. M., Darin K. M., Scarsi K. K., et al. Antiretroviral pharmacokinetics in pregnant women. Pharmacotherapy 2015;35(9):838-55. [PMID: 26297552]
Gonzalez de Requena D., Bonora S., Viganò O., et al. Comparative evaluation of seven resistance interpretation algorithms and their derived genotypic inhibitory quotients for the prediction of 48 week virological response to darunavir-based salvage regimens. J Antimicrob Chemother 2011;66(1):192-200. [PMID: 21037251]
Gonzalez-Serna A., Glas A. C., Brumme C. J., et al. Genotypic susceptibility score (GSS) and CD4+ T cell recovery in HIV-1 patients with suppressed viral load. J Antimicrob Chemother 2017;72(2):496-503. [PMID: 27999069]
Gulick R. M., Lalezari J., Goodrich J., et al. Maraviroc for previously treated patients with R5 HIV-1 infection. N Engl J Med 2008;359(14):1429-41. [PMID: 18832244]
Gutiérrez C., Díaz L., Vallejo A., et al. Intensification of antiretroviral therapy with a CCR5 antagonist in patients with chronic HIV-1 infection: effect on T cells latently infected. PLoS One 2011;6(12):e27864. [PMID: 22174752]
Hagins D., Orkin C., Daar E. S., et al. Switching to coformulated rilpivirine (RPV), emtricitabine (FTC) and tenofovir alafenamide from either RPV, FTC and tenofovir disoproxil fumarate (TDF) or efavirenz, FTC and TDF: 96-week results from two randomized clinical trials. HIV Med 2018;19(10):724-33. [PMID: 30101539]
Halvas E. K., Aga E., Bosch R. J., et al. Variable persistence of non-suppressible viremia on antiretroviral therapy. Abstract 473. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/variable-persistence-of-non-suppressible-viremia-on-antiretroviral-therapy/
Halvas E. K., Joseph K. W., Brandt L. D., et al. HIV-1 viremia not suppressible by antiretroviral therapy can originate from large T cell clones producing infectious virus. J Clin Invest 2020;130(11):5847-57. [PMID: 33016926]
Havlir D. V., Bassett R., Levitan D., et al. Prevalence and predictive value of intermittent viremia with combination HIV therapy. JAMA 2001;286(2):171-79. [PMID: 11448280]
Hayashida T., Hachiya A., Ode H., et al. Rilpivirine resistance mutation E138K in HIV-1 reverse transcriptase predisposed by prevalent polymorphic mutations. J Antimicrob Chemother 2016;71(10):2760-66. [PMID: 27330069]
Hickey M., Grochowski J., Mayorga-Munoz F., et al. 24-Week viral suppression in patients starting long-acting CAB/RPV without HIV viral suppression. Abstract 628. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/24-week-viral-suppression-in-patients-starting-long-acting-cab-rpv-without-hiv-viral-suppression/
Hickey M. D., Gistand N., Grochowski J., et al. Viral suppression rates at 48 weeks in people with HIV starting long-acting cabotegravir/rilpivirine with initial viremia. Clin Infect Dis 2025;80(4):864-870. [PMID: 39367871]
Hoffmann C., Welz T., Sabranski M., et al. Higher rates of neuropsychiatric adverse events leading to dolutegravir discontinuation in women and older patients. HIV Med 2017;18(1):56-63. [PMID: 27860104]
Holt S. G., Gracey D. M., Levy M. T., et al. A consensus statement on the renal monitoring of Australian patients receiving tenofovir based antiviral therapy for HIV/HBV infection. AIDS Res Ther 2014;11:35. [PMID: 25745499]
Houston E., Osborn A., Lyons T., et al. Exploring perceived social support from peer facilitators in an HIV treatment adherence intervention for African American patients: a content analysis of participant perspectives. J Commun Appl Soc Psychol 2015;25(6):487-501. https://doi.org/10.1002/casp.2228
Hunt P. W., Shulman N. S., Hayes T. L., et al. The immunologic effects of maraviroc intensification in treated HIV-infected individuals with incomplete CD4+ T-cell recovery: a randomized trial. Blood 2013;121(23):4635-46. [PMID: 23589670]
Iarikov D. E., Irizarry-Acosta M., Martorell C., et al. Use of HIV resistance testing after prolonged treatment interruption. J Acquir Immune Defic Syndr 2010;53(3):333-37. [PMID: 20009764]
Inzaule S. C., Hamers R. L., Noguera-Julian M., et al. Clinically relevant thresholds for ultrasensitive HIV drug resistance testing: a multi-country nested case-control study. Lancet HIV 2018;5(11):e638-46. [PMID: 30282603]
Jacobs J. L., Halvas E. K., Tosiano M. A., et al. Persistent HIV-1 viremia on antiretroviral therapy: measurement and mechanisms. Front Microbiol 2019;10:2383. [PMID: 31681237]
Jaschinski N., Greenberg L., Neesgaard B., et al. Recent abacavir use and incident cardiovascular disease in contemporary-treated people with HIV. AIDS 2023;37(3):467-75. [PMID: 36001525]
Johnson M., Kumar P., Molina J. M., et al. Switching to roravirine/lamivudine/tenofovir disoproxil fumarate (DOR/3TC/TDF) maintains HIV-1 virologic suppression through 48 weeks: results of the DRIVE-SHIFT trial. J Acquir Immune Defic Syndr 2019;81(4):463-72. [PMID: 30985556]
Jones L. E., Perelson A. S. Opportunistic infection as a cause of transient viremia in chronically infected HIV patients under treatment with HAART. Bull Math Biol 2005;67(6):1227-51. [PMID: 16023709]
Juárez-González J. A., Sanchez Cruz E. I., Angulo-Medina L. A., et al. Resistance to second-generation InSTIs in Mexican PLWH: emergence of the R263K mutant. Abstract 679. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/resistance-to-second-generation-instis-in-mexican-plwh-emergence-of-the-r263k-mutant/
Jülg B., Goebel F. D. Treatment interruption in HIV therapy: a SMART strategy?. Infection 2006;34(3):186-88. [PMID: 16804667]
Kabra M., Barber T. J., Allavena C., et al. Effectiveness of dolutegravir + lamivudine in real-world studies in people with HIV-1 with M184V/I mutations: a systematic review and meta-analysis. HIV Glasgow; 2022 Oct 23-26; Virtual. https://www.natap.org/2022/Glascow/GLASGOW_65.htm
Kanters S., Vitoria M., Zoratti M., et al. Comparative efficacy, tolerability and safety of dolutegravir and efavirenz 400mg among antiretroviral therapies for first-line HIV treatment: a systematic literature review and network meta-analysis. EClinicalMedicine 2020;28:100573. [PMID: 33294805]
Katlama C., Clotet B., Mills A., et al. Efficacy and safety of etravirine at week 96 in treatment-experienced HIV type-1-infected patients in the DUET-1 and DUET-2 trials. Antivir Ther 2010;15(7):1045-52. [PMID: 21041921]
Kearney M. F., Spindler J., Shao W., et al. Lack of detectable HIV-1 molecular evolution during suppressive antiretroviral therapy. PLoS Pathog 2014;10(3):e1004010. [PMID: 24651464]
Kim S. H., Gerver S. M., Fidler S., et al. Adherence to antiretroviral therapy in adolescents living with HIV: systematic review and meta-analysis. AIDS 2014;28(13):1945-56. [PMID: 24845154]
Kingwara L., Onwonga V. M., Madada R. S., et al. DTG resistance in patients with previous ARV experience and viremia in Kenya receiving DTG-based ART. Abstract 677. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/dtg-resistance-in-patients-with-previous-arv-experience-and-viremia-in-kenya-receiving-dtg-based-art/
Kityo C., Mambule I. K., Musaazi J., et al. Switch to long-acting cabotegravir and rilpivirine in virologically suppressed adults with HIV in Africa (CARES): week 48 results from a randomised, multicentre, open-label, non-inferiority trial. Lancet Infect Dis 2024;24(10):1083-92. [PMID: 38821073]
Kozal M., Aberg J., Pialoux G., et al. Fostemsavir in adults with multidrug-resistant HIV-1 infection. N Engl J Med 2020;382(13):1232-43. [PMID: 32212519]
Kumar P., Johnson M., Molina J. M., et al. Brief report: switching to DOR/3TC/TDF maintains HIV-1 virologic suppression through week 144 in the DRIVE-SHIFT trial. J Acquir Immune Defic Syndr 2021;87(2):801-5. [PMID: 33633036]
Landovitz R. J., Li S., Eron J. J., et al. Tail-phase safety, tolerability, and pharmacokinetics of long-acting injectable cabotegravir in HIV-uninfected adults: a secondary analysis of the HPTN 077 trial. Lancet HIV 2020;7(7):e472-81. [PMID: 32497491]
Lataillade M., Zhou N., Joshi S. R., et al. Viral drug resistance through 48 weeks, in a phase 2b, randomized, controlled trial of the HIV-1 attachment inhibitor prodrug, fostemsavir. J Acquir Immune Defic Syndr 2018;77(3):299-307. [PMID: 29206721]
Lathouwers E., Wong E. Y., Luo D., et al. HIV-1 resistance rarely observed in patients using darunavir once-daily regimens across clinical studies. HIV Clin Trials 2017;18(5-6):196-204. [PMID: 29143565]
Lederman M. M., Calabrese L., Funderburg N. T., et al. Immunologic failure despite suppressive antiretroviral therapy is related to activation and turnover of memory CD4 cells. J Infect Dis 2011;204(8):1217-26. [PMID: 21917895]
Lewden C., Bouteloup V., De Wit S., et al. All-cause mortality in treated HIV-infected adults with CD4. Int J Epidemiol 2012;41(2):433-45. [PMID: 22493325]
Li Y., Etemad B., Dele-Oni R., et al. Drug resistance mutations in HIV provirus are associated with defective proviral genomes with hypermutation. AIDS 2021;35(7):1015-20. [PMID: 33635848]
Llibre J. M., Brites C., Cheng C. Y., et al. Efficacy and safety of switching to the 2-drug regimen dolutegravir/lamivudine versus continuing a 3- or 4-drug regimen for maintaining virologic suppression in adults living with HIV-1: week 48 results from the phase 3, non-inferiority SALSA randomized trial. Clin Infect Dis 2022;76(4):720-29. [PMID: 35235656]
Llibre J. M., Hung C. C., Brinson C., et al. Efficacy, safety, and tolerability of dolutegravir-rilpivirine for the maintenance of virological suppression in adults with HIV-1: phase 3, randomised, non-inferiority SWORD-1 and SWORD-2 studies. Lancet 2018;391(10123):839-49. [PMID: 29310899]
Luber A. D. Genetic barriers to resistance and impact on clinical response. MedGenMed 2005;7(3):69. [PMID: 16369295]
Lynch T., Price A. The effect of cytochrome P450 metabolism on drug response, interactions, and adverse effects. Am Fam Physician 2007;76(3):391-96. [PMID: 17708140]
Magambo B., Nazziwa J., Bbosa N., et al. The arrival of untreatable multidrug-resistant HIV-1 in sub-Saharan Africa. AIDS 2014;28(9):1373-74. [PMID: 24959965]
Maggiolo F., Gianotti N., Comi L., et al. Rilpivirine plus cobicistat-boosted darunavir as alternative to standard three-drug therapy in HIV-infected, virologically suppressed subjects: final results of the PROBE 2 trial. Antivir Ther 2021;26(3-5):51-57. [PMID: 35485333]
Mallon P. W., Brunet L., Hsu R. K., et al. Weight gain before and after switch from TDF to TAF in a U.S. cohort study. J Int AIDS Soc 2021;24(4):e25702. [PMID: 33838004]
Marcelin A. G., Masquelier B., Descamps D., et al. Tipranavir-ritonavir genotypic resistance score in protease inhibitor-experienced patients. Antimicrob Agents Chemother 2008;52(9):3237-43. [PMID: 18625773]
Margot N. A., Jogiraju V., Pennetzdorfer N., et al. Resistance analyses in heavily treatment-experienced people with HIV treated with the novel HIV capsid inhibitor lenacapavir after 2 years. J Infect Dis 2025;231:1239-45. [PMID: 39873394]
Matthews G., Borok M., Eriobou N., et al. D2EFT: dolutegravir and darunavir evaluation in adults failing first-line HIV therapy. Abstract 198. CROI; 2023 Feb 19-22; Seattle, WA. https://www.croiconference.org/abstract/d2eft-dolutegravir-and-darunavir-evaluation-in-adults-failing-first-line-hiv-therapy/
Matveev V. A., Mihelic E. Z., Benko E., et al. Immunogenicity of COVID-19 vaccines and their effect on HIV reservoir in older people with HIV. iScience 2023;26(10):107915. [PMID: 37790281]
McClung R. P., Oster A. M., Ocfemia M. C. B., et al. Transmitted drug resistance among human immunodeficiency virus (HIV)-1 diagnoses in the United States, 2014-2018. Clin Infect Dis 2022;74(6):1055-62. [PMID: 34175948]
McMahon D., Jones J., Wiegand A., et al. Short-course raltegravir intensification does not reduce persistent low-level viremia in patients with HIV-1 suppression during receipt of combination antiretroviral therapy. Clin Infect Dis 2010;50(6):912-19. [PMID: 20156060]
Mills A., Arribas J. R., Andrade-Villanueva J., et al. Switching from tenofovir disoproxil fumarate to tenofovir alafenamide in antiretroviral regimens for virologically suppressed adults with HIV-1 infection: a randomised, active-controlled, multicentre, open-label, phase 3, non-inferiority study. Lancet Infect Dis 2016;16(1):43-52. [PMID: 26538525]
Mohammadi A., Etemad B., Zhang X., et al. Viral and host mediators of non-suppressible HIV-1 viremia. Nat Med 2023;29(12):3212-23. [PMID: 37957382]
Molina J. M., Ward D., Brar I., et al. Switching to fixed-dose bictegravir, emtricitabine, and tenofovir alafenamide from dolutegravir plus abacavir and lamivudine in virologically suppressed adults with HIV-1: 48 week results of a randomised, double-blind, multicentre, active-controlled, phase 3, non-inferiority trial. Lancet HIV 2018;5(7):e357-65. [PMID: 29925489]
Mosier D. E. How HIV changes its tropism: evolution and adaptation?. Curr Opin HIV AIDS 2009;4(2):125-30. [PMID: 19339951]
Mulenga L. B., Fwoloshi S., Mweemba A., et al. Dolutegravir with recycled nRTIs is noninferior to PI-based ART: VISEND trial. Abstract 135. CROI; 2022 Feb 12-16; Virtual. https://www.croiconference.org/abstract/dolutegravir-with-recycled-nrtis-is-noninferior-to-pi-based-art-visend-trial/
Napravnik S., Keys J. R., Quinlivan E. B., et al. Triple-class antiretroviral drug resistance: risk and predictors among HIV-1-infected patients. AIDS 2007;21(7):825-34. [PMID: 17415037]
Noe A., Plum J., Verhofstede C. The latent HIV-1 reservoir in patients undergoing HAART: an archive of pre-HAART drug resistance. J Antimicrob Chemother 2005;55(4):410-12. [PMID: 15728140]
Ogbuagu O., Ratanasuwan W., Avihingsanon A., et al. Lenacapavir efficacy in CAPELLA patients with no fully active agents in optimized background regimen. Abstract 630. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/lenacapavir-efficacy-in-capella-patients-with-no-fully-active-agents-in-optimized-background-regimen/
Ogbuagu(a) O., Segal-Maurer S., Ratanasuwan W., et al. Efficacy and safety of the novel capsid inhibitor lenacapavir to treat multidrug-resistant HIV: week 52 results of a phase 2/3 trial. Lancet HIV 2023;10(8):e497-505. [PMID: 37451297]
Ogbuagu(b) O. Week 52 subgroup efficacy of lenacapavir in heavily treatment-experienced PWH. Abstract 523. CROI; 2023 Feb 19-22; Seattle, WA. https://www.croiconference.org/abstract/week-52-subgroup-efficacy-of-lenacapavir-in-heavily-treatment-experienced-pwh/
Oliveira M., Ibanescu R. I., Anstett K., et al. Selective resistance profiles emerging in patient-derived clinical isolates with cabotegravir, bictegravir, dolutegravir, and elvitegravir. Retrovirology 2018;15(1):56. [PMID: 30119633]
Ombajo L. A., Penner J., Nkuranga J., et al. Second-line switch to dolutegravir for treatment of HIV infection. N Engl J Med 2023;388(25):2349-59. [PMID: 37342923]
Orkin C., Arasteh K., Gorgolas Hernandez-Mora M., et al. Long-acting cabotegravir and rilpivirine after oral induction for HIV-1 infection. N Engl J Med 2020;382(12):1124-35. [PMID: 32130806]
Orkin C., DeJesus E., Ramgopal M., et al. Switching from tenofovir disoproxil fumarate to tenofovir alafenamide coformulated with rilpivirine and emtricitabine in virally suppressed adults with HIV-1 infection: a randomised, double-blind, multicentre, phase 3b, non-inferiority study. Lancet HIV 2017;4(5):e195-204. [PMID: 28259777]
Orkin C., Schapiro J. M., Perno C. F., et al. Expanded multivariable models to assist patient selection for long-acting cabotegravir + rilpivirine treatment: clinical utility of a combination of patient, drug concentration, and viral factors associated with virologic failure. Clin Infect Dis 2023;77(10):1423-31. [PMID: 37340869]
Orta-Resendiz A., Rodriguez-Diaz R. A., Angulo-Medina L. A., et al. HIV-1 acquired drug resistance to integrase inhibitors in a cohort of antiretroviral therapy multi-experienced Mexican patients failing to raltegravir: a cross-sectional study. AIDS Res Ther 2020;17(1):6. [PMID: 32041622]
Ortego C., Huedo-Medina T. B., Llorca J., et al. Adherence to highly active antiretroviral therapy (HAART): a meta-analysis. AIDS Behav 2011;15(7):1381-96. [PMID: 21468660]
Overton E. T., Richmond G., Rizzardini G., et al. Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with HIV-1 infection (ATLAS-2M), 48-week results: a randomised, multicentre, open-label, phase 3b, non-inferiority study. Lancet 2021;396(10267):1994-2005. [PMID: 33308425]
Palella F. J., Fisher M., Tebas P., et al. Simplification to rilpivirine/emtricitabine/tenofovir disoproxil fumarate from ritonavir-boosted protease inhibitor antiretroviral therapy in a randomized trial of HIV-1 RNA-suppressed participants. AIDS 2014;28(3):335-44. [PMID: 24670520]
Papageorgiou V., Davies B., Cooper E., et al. Influence of material deprivation on clinical outcomes among people living with HIV in high-income countries: a systematic review and meta-analysis. AIDS Behav 2022;26(6):2026-54. [PMID: 34894331]
Paton N. I., Musaazi J., Kityo C., et al. Efficacy and safety of dolutegravir or darunavir in combination with lamivudine plus either zidovudine or tenofovir for second-line treatment of HIV infection (NADIA): week 96 results from a prospective, multicentre, open-label, factorial, randomised, non-inferiority trial. Lancet HIV 2022;9(6):e381-93. [PMID: 35460601]
Plum P. E., Maes N., Sauvage A. S., et al. Impact of switch from tenofovir disoproxil fumarate-based regimens to tenofovir alafenamide-based regimens on lipid profile, weight gain and cardiovascular risk score in people living with HIV. BMC Infect Dis 2021;21(1):910. [PMID: 34488664]
Prabhakar B., Banu A., Pavithra H. B., et al. Immunological failure despite virological suppression in HIV seropositive individuals on antiretroviral therapy. Indian J Sex Transm Dis AIDS 2011;32(2):94-98. [PMID: 22021970]
Puertas M. C., Ploumidis G., Ploumidis M., et al. Pan-resistant HIV-1 emergence in the era of integrase strand-transfer inhibitors: a case report. Lancet Microbe 2020;1(3):e130-35. [PMID: 35544263]
Raccagni A. R., Diotallevi S., Lolatto R., et al. Viral blips and virologic failures following mpox vaccination with MVA-BN among people with HIV. AIDS 2023;37(15):2365-69. [PMID: 37773029]
Rana A. I., Bao Y., Zheng L., et al. Long-acting injectable CAB/RPV is superior to oral ART in PWH with adherence challenges: ACTG A5359. Abstract 212. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/long-acting-injectable-cab-rpv-is-superior-to-oral-art-in-pwh-with-adherence-challenges-actg-a5359/
Rathbun C., Liedtke M. D. The next generation: etravirine in the treatment of HIV-1 infection in adults refractory to other antiretrovirals. Virus Adapt Treat 2010;2:91-102. https://doi.org/10.2147/VAAT.S6413
Ratouit P., Guiraud V., Malet I., et al. HIV-1 resistance mutations to integrase inhibitors impair both integration and reverse transcription. Abstract 684. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/hiv-1-resistance-mutations-to-integrase-inhibitors-impair-both-integration-and-reverse-transcription/
Riddler S. A., Haubrich R., DiRienzo A. G., et al. Class-sparing regimens for initial treatment of HIV-1 infection. N Engl J Med 2008;358(20):2095-2106. [PMID: 18480202]
Rizzardini G., Overton E. T., Orkin C., et al. Long-acting injectable cabotegravir + rilpivirine for HIV maintenance therapy: week 48 pooled analysis of phase 3 ATLAS and FLAIR trials. J Acquir Immune Defic Syndr 2020;85(4):498-506. [PMID: 33136751]
Ryan P., Blanco J. L., Masi M. , et al. Non-inferior efficacy and less weight gain when switching to DTG/3TC than when switching to BIC/FTC/TAF in virologically suppressed people with HIV (PWH): the PASO-DOBLE (GeSIDA 11720) randomized clinical trial. Abstract OAB3606LB. 25th International AIDS Conference; 2024 Jul 22-26; Munich, Germany. https://doi.org/10.1002/jia2.26279
Ryom L., Lundgren J. D., El-Sadr W., et al. Cardiovascular disease and use of contemporary protease inhibitors: the D:A:D international prospective multicohort study. Lancet HIV 2018;5(6):e291-300. [PMID: 29731407]
Ryscavage P., Kelly S., Li J. Z., et al. Significance and clinical management of persistent low-level viremia and very-low-level viremia in HIV-1-infected patients. Antimicrob Agents Chemother 2014;58(7):3585-98. [PMID: 24733471]
Sabin C. A., Ryom L., d'Arminio Monforte A., et al. Abacavir use and risk of recurrent myocardial infarction. AIDS 2018;32(1):79-88. [PMID: 29028664]
Santos J. R., Domingo P., Portilla J., et al. A randomized trial of dolutegravir plus darunavir/cobicistat as a switch strategy in HIV-1-infected patients with resistance to at least 2 antiretroviral classes. Open Forum Infect Dis 2023;10(11):ofad542. [PMID: 38023553]
Sax P. E., Andreatta K., Molina J. M., et al. High efficacy of switching to bictegravir/emtricitabine/tenofovir alafenamide in people with suppressed HIV and preexisting M184V/I. AIDS 2022;36(11):1511-20. [PMID: 35466963]
Sax(a) P. E., Rockstroh J. K., Luetkemeyer A. F., et al. Switching to bictegravir, emtricitabine, and tenofovir alafenamide in virologically suppressed adults with HIV. Clin Infect Dis 2020;73(2):e485-93. [PMID: 32668455]
Sax(b) P. E., Erlandson K. M., Lake J. E., et al. Weight gain following initiation of antiretroviral therapy: risk factors in randomized comparative clinical trials. Clin Infect Dis 2020;71(6):1379-89. [PMID: 31606734]
Schaecher K. L. The importance of treatment adherence in HIV. Am J Manag Care 2013;19(12 Suppl):s231-37. [PMID: 24495293]
Schapiro J. M., Kaiser R., Krystal M., et al. Fostemsavir resistance in clinical context: a narrative review. Ther Adv Infect Dis 2025;12:20499361251325103. [PMID: 40145022]
Scherrer A. U., von Wyl V., Böni J., et al. Viral suppression rates in salvage treatment with raltegravir improved with the administration of genotypic partially active or inactive nucleoside/tide reverse transcriptase inhibitors. J Acquir Immune Defic Syndr 2011;57(1):24-31. [PMID: 21283013]
Sedaghat A. R., Dinoso J. B., Shen L., et al. Decay dynamics of HIV-1 depend on the inhibited stages of the viral life cycle. Proc Natl Acad Sci U S A 2008;105(12):4832-37. [PMID: 18362342]
Segal-Maurer S., DeJesus E., Stellbrink H. J., et al. Capsid inhibition with lenacapavir in multidrug-resistant HIV-1 infection. N Engl J Med 2022;386(19):1793-1803. [PMID: 35544387]
Shafer R. W., Schapiro J. M. HIV-1 drug resistance mutations: an updated framework for the second decade of HAART. AIDS Rev 2008;10(2):67-84. [PMID: 18615118]
Skrivankova V.W., Huwa J., Muula G., et al. Viremia and drug resistance 2 years after routine switching to dolutegravir-based first-line ART. Abstract 676. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/viremia-and-drug-resistance-2-years-after-routine-switching-to-dolutegravir-based-first-line-art/
Squillace N., Ricci E., Menzaghi B., et al. The effect of switching from tenofovir disoproxil fumarate (TDF) to tenofovir alafenamide (TAF) on liver enzymes, glucose, and lipid profile. Drug Des Devel Ther 2020;14:5515-20. [PMID: 33364747]
Steigbigel R. T., Cooper D. A., Kumar P. N., et al. Raltegravir with optimized background therapy for resistant HIV-1 infection. N Engl J Med 2008;359(4):339-54. [PMID: 18650512]
Surial B., Mugglin C., Calmy A., et al. Weight and metabolic changes after switching from tenofovir disoproxil fumarate to tenofovir alafenamide in people living with HIV: a cohort study. Ann Intern Med 2021;174(6):758-67. [PMID: 33721521]
Swenson L. C., Min J. E., Woods C. K., et al. HIV drug resistance detected during low-level viraemia is associated with subsequent virologic failure. AIDS 2014;28(8):1125-34. [PMID: 24451160]
Swindells S., Andrade-Villanueva J. F., Richmond G. J., et al. Long-acting cabotegravir and rilpivirine for maintenance of HIV-1 suppression. N Engl J Med 2020;382(12):1112-23. [PMID: 32130809]
Tang M. W., Shafer R. W. HIV-1 antiretroviral resistance: scientific principles and clinical applications. Drugs 2012;72(9):e1-25. [PMID: 22686620]
Tashima K. T., Mollan K. R., Na L., et al. Regimen selection in the OPTIONS trial of HIV salvage therapy: drug resistance, prior therapy, and race-ethnicity determine the degree of regimen complexity. HIV Clin Trials 2015;16(4):147-56. [PMID: 26212575]
Teira R., Vidal F., Muñoz-Sánchez P., et al. Very low level viraemia and risk of virological failure in treated HIV-1-infected patients. HIV Med 2017;18(3):196-203. [PMID: 27476742]
Tiraboschi J., Crusells M. J., Domingo P.Guerri-Fernandez, et al. Switch to DTG/3TC vs B/F/TAF (PASO-DOBLE Study): efficacy and weight changes by predefined subgroups. Abstract 661. CROI; 2025 Mar 9-12; San Francisco, CA. https://www.croiconference.org/abstract/1035-2025/
Trottier B., Lake J. E., Logue K., et al. Dolutegravir/abacavir/lamivudine versus current ART in virally suppressed patients (STRIIVING): a 48-week, randomized, non-inferiority, open-label, Phase IIIb study. Antivir Ther 2017;22(4):295-305. [PMID: 28401876]
Tsiodras S., Mantzoros C., Hammer S., et al. Effects of protease inhibitors on hyperglycemia, hyperlipidemia, and lipodystrophy: a 5-year cohort study. Arch Intern Med 2000;160(13):2050-56. [PMID: 10888979]
University of Liverpool. Food considerations for antiretrovirals. 2016 Mar. https://liverpool-hiv-hep.s3.amazonaws.com/treatment_selectors/pdfs/000/000/021/original/ARV_Food_2016_Mar.pdf?1512551709 [accessed 2025 May 6]
Van Dyke R. B., Patel K., Kagan R. M., et al. Antiretroviral drug resistance among children and youth in the United States with perinatal HIV. Clin Infect Dis 2016;63(1):133-37. [PMID: 27056398]
van Wyk J., Ajana F., Bisshop F., et al. Efficacy and safety of switching to dolutegravir/lamivudine fixed-dose 2-drug regimen vs continuing a tenofovir alafenamide-based 3- or 4-drug regimen for maintenance of virologic suppression in adults living with human immunodeficiency virus type 1: phase 3, randomized, noninferiority TANGO study. Clin Infect Dis 2020;71(8):1920-29. [PMID: 31905383]
Vandenhende M. A., Ingle S., May M., et al. Impact of low-level viremia on clinical and virological outcomes in treated HIV-1-infected patients. AIDS 2015;29(3):373-83. [PMID: 25686685]
Venter W. D. F., Moorhouse M., Sokhela S., et al. Dolutegravir plus two different prodrugs of tenofovir to treat HIV. N Engl J Med 2019;381(9):803-15. [PMID: 31339677]
Vingerhoets J., Tambuyzer L., Azijn H., et al. Resistance profile of etravirine: combined analysis of baseline genotypic and phenotypic data from the randomized, controlled phase III clinical studies. AIDS 2010;24(4):503-14. [PMID: 20051805]
Wainberg M. A. The impact of the M184V substitution on drug resistance and viral fitness. Expert Rev Anti Infect Ther 2004;2(1):147-51. [PMID: 15482179]
Wallis C. L., McCarthy C., Godfrey C., et al. ACTG 5381: virologic and resistance outcomes after switch to TLD for failing 1st- or 2nd-line ART. Abstract 675. CROI; 2024 Mar 3-6; Denver, CO. https://www.croiconference.org/abstract/actg-5381-virologic-and-resistance-outcomes-after-switch-to-tld-for-failing-1st-or-2nd-line-art/
Wang H., Lu X., Yang X., et al. The efficacy and safety of tenofovir alafenamide versus tenofovir disoproxil fumarate in antiretroviral regimens for HIV-1 therapy: meta-analysis. Medicine (Baltimore) 2016;95(41):e5146. [PMID: 27741146]
Waters L., Bansi L., Asboe D., et al. Second-line protease inhibitor-based antiretroviral therapy after non-nucleoside reverse transcriptase inhibitor failure: the effect of a nucleoside backbone. Antivir Ther 2013;18(2):213-19. [PMID: 23653911]
Weinstein M. C., Goldie S. J., Losina E., et al. Use of genotypic resistance testing to guide HIV therapy: clinical impact and cost-effectiveness. Ann Intern Med 2001;134(6):440-50. [PMID: 11255519]
Wensing A. M., Charpentier C., Calvez V., et al. Utilizing HIV proviral DNA to assess for the presence of HIV drug resistance. Clin Infect Dis 2025. [PMID: 40176204]
WHO. WHO recommends dolutegravir as preferred HIV treatment option in all populations. 2019 Jul 22. https://www.who.int/news/item/22-07-2019-who-recommends-dolutegravir-as-preferred-hiv-treatment-option-in-all-populations [accessed 2025 May 6]
Wirden M., Pouderoux C., Peytavin G., et al. Ultra-rapid selection of the N74D capsid inhibitor resistance mutation after 3 weeks on lenacapavir. J Antimicrob Chemother 2024;79(7):1706-7. [PMID: 38629483]
Yombi J. C. Dolutegravir neuropsychiatric adverse events: specific drug effect or class effect. AIDS Rev 2018;20(1):14-26. [PMID: 29628511]
Younas M., Psomas C., Reynes C., et al. Residual viremia is linked to a specific immune activation profile in HIV-1-infected adults under efficient antiretroviral therapy. Front Immunol 2021;12:663843. [PMID: 33859653]
Yukawa S., Watanabe D., Uehira T., et al. Clinical benefits of using inulin clearance and cystatin C for determining glomerular filtration rate in HIV-1-infected individuals treated with dolutegravir. J Infect Chemother 2018;24(3):199-205. [PMID: 29150412]
Zash R., Holmes L. B., Diseko M., et al. Update on neural tube defects with antiretroviral exposure in the Tsepamo Study, Botswana. 24th International AIDS Conference; 2022 Jul 29-Aug 1; Montreal, Canada. https://www.natap.org/2022/IAC/IAC_31.htm
Updates, Authorship, and Related Guidelines
| Updates, Authorship, and Related Guidelines | |
| Date of original publication | November 29, 2022 |
| Date of current publication | February 10, 2026 |
| Highlights of changes, additions, and updates in the February 10, 2026 edition |
|
| Intended users | Clinicians who treat patients with HIV who require changes in their ART regimens |
| Lead author |
Joseph P. McGowan, MD, FACP, FIDSA, AAHIVS |
| Writing group |
Rona M. Vail, MD, AAHIVS; Sanjiv S. Shah, MD, MPH, AAHIVS; Steven M. Fine, MD, PhD; Samuel T. Merrick, MD, FIDSA; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Jessica Rodrigues, MPH, MS; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD; Christopher J. Hoffmann, MD, MPH, MSc, FACP |
| Author and writing group conflict of interest disclosures | There are no author or writing group conflict of interest disclosures. |
| Committee | |
| Developer and funder |
New York State Department of Health AIDS Institute (NYSDOH AI) |
| Development process |
See Guideline Development and Recommendation Ratings Scheme, below. |
| Related NYSDOH AI guidelines |
Guidelines
GuidancePodcast |
Guideline Development and Recommendation Ratings
| Guideline Development: New York State Department of Health AIDS Institute Clinical Guidelines Program | |
| Program manager | Clinical Guidelines Program, Johns Hopkins University School of Medicine, Division of Infectious Diseases. See Program Leadership and Staff. |
| Mission | To produce and disseminate evidence-based, state-of-the-art clinical practice guidelines that establish uniform standards of care for practitioners who provide prevention or treatment of HIV, viral hepatitis, other sexually transmitted infections, and substance use disorders for adults throughout New York State in the wide array of settings in which those services are delivered. |
| Expert committees | The NYSDOH AI Medical Director invites and appoints committees of clinical and public health experts from throughout New York State to ensure that the guidelines are practical, immediately applicable, and meet the needs of care providers and stakeholders in all major regions of New York State, all relevant clinical practice settings, key New York State agencies, and community service organizations. |
| Committee structure |
|
| Disclosure and management of conflicts of interest |
|
| Evidence collection and review |
|
| Recommendation development |
|
| Review and approval process |
|
| External reviews |
|
| Update process |
|
| Recommendation Ratings Scheme | |||
| Strength | Quality of Evidence | ||
| Rating | Definition | Rating | Definition |
| A | Strong | 1 | Based on published results of at least 1 randomized clinical trial with clinical outcomes or validated laboratory endpoints. |
| B | Moderate | * | Based on either a self-evident conclusion; conclusive, published, in vitro data; or well-established practice that cannot be tested because ethics would preclude a clinical trial. |
| C | Optional | 2 | Based on published results of at least 1 well-designed, nonrandomized clinical trial or observational cohort study with long-term clinical outcomes. |
| 2† | Extrapolated from published results of well-designed studies (including nonrandomized clinical trials) conducted in populations other than those specifically addressed by a recommendation. The source(s) of the extrapolated evidence and the rationale for the extrapolation are provided in the guideline text. One example would be results of studies conducted predominantly in a subpopulation (e.g., one gender) that the committee determines to be generalizable to the population under consideration in the guideline. | ||
| 3 | Based on committee expert opinion, with rationale provided in the guideline text. | ||
Last updated on March 18, 2026