
Purpose of This Guideline
Date of current publication: June 10, 2026
Lead author: Daniela E. DiMarco, MD, MPH
Writing group: Rona M. Vail, MD, AAHIVS; Sanjiv S. Shah, MD, MPH, AAHIVS; Steven M. Fine, MD, PhD; Joseph P. McGowan, MD, FACP, FIDSA, AAHIVS; Samuel T. Merrick, MD, FIDSA; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Anne K. Monroe, MD, MSPH; Marguerite A. Urban, MD; Jessica Rodrigues, MPH, MS; Brianna L. Norton, DO, MPH; Christopher J. Hoffmann, MD, MPH, MSc, FACP; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: September 28, 2020
The New York State Department of Health AIDS Institute (NYSDOH AI) Clinical Guidelines Program developed this guideline to address the care of adults with and without HIV who have acquired sexually transmitted Mycoplasma genitalium infection, with the goals of:
- Assisting clinicians in recognizing common clinical manifestations of M. genitalium infection
- Providing clinicians with evidence-based recommendations on screening, diagnostic testing, and treatment of M. genitalium infection
- Ensuring New York State recommendations for M. genitalium screening, diagnosis, and treatment reflect the rapidly evolving evidence on the organism, infection, potential complications, and implications of drug resistance
M. genitalium is a well-recognized cause of sexually transmitted infections (STIs) worldwide and is linked to urethritis, cervicitis, and pelvic inflammatory disease, yet much is still unknown about the organism, infection, and potential complications. Treatment of M. genitalium infection is challenging in an era of increasing antimicrobial resistance across multiple drug classes. Emerging antimicrobial resistance worldwide has become a concern, and specific testing strategies and treatment recommendations in the United States and elsewhere have been implemented to address this issue.
Prevalence of M. genitalium infection: The prevalence of M. genitalium infection varies depending on the clinical setting and population being tested. In a large U.S. cohort of participants with and without STI symptoms in varied clinical settings, overall M. genitalium prevalence was approximately 10% Gaydos, et al. 2019. In the MyGeniUS study, which examined M. genitalium prevalence and resistance mutations in STI clinics across the United States, overall prevalence was slightly higher at 16.6% Manhart, et al. 2023. Prevalence has consistently been higher among individuals younger than 21 years Manhart, et al. 2023; Menezes, et al. 2023. M. genitalium prevalence among people with HIV in North America is estimated to be 20% Zhang, et al. 2025. Data from multiple countries and populations that include a mix of symptomatic and asymptomatic individuals suggest that asymptomatic M. genitalium infection is common Calas, et al. 2021; Gesink, et al. 2016; Huppert, et al. 2008; Manhart, et al. 2007.
Clinical Manifestations
Although asymptomatic infection is common, Mycoplasma genitalium infection has been associated with the clinical syndromes of urethritis, cervicitis, and pelvic inflammatory disease (PID). The relationships between M. genitalium and cervicitis and urethritis have been established, with the strongest association seen with urethritis CDC 2021; Dehon, et al. 2016; Lis, et al. 2015; Lusk, et al. 2011; Gaydos, et al. 2009; Wikström and Jensen 2006; Mena, et al. 2002; Totten, et al. 2001. Symptoms are typically similar to those seen with chlamydial urethritis (nonpurulent urethral discharge) as opposed to gonococcal urethritis (frankly purulent discharge).
A 2023 systematic review and meta-analysis found that M. genitalium, detected by nucleic acid amplification testing, was associated with 67% greater odds of PID Htaik, et al. 2024. A randomized trial comparing the addition of metronidazole or placebo to standard PID treatment (ceftriaxone plus doxycycline) noted a statistically significant reduction in detection of M. genitalium 30 days after treatment in the metronidazole arm Wiesenfeld, et al. 2021. More recently, in a study conducted in sexually transmitted infection clinics in the United States, infection with M. genitalium was associated with bacterial vaginosis (odds ratio, 3.08; 95% confidence interval, 1.58–5.99, P=.0113), although control for other factors associated with BV was limited Schwebke, et al. 2024. Some experts suggest these findings implicate the influence of the vaginal microbiome on M. genitalium, but further investigation is needed Mitchell, et al. 2021.
M. genitalium has been identified at various anatomic sites Baiers, et al. 2024; Yazdy, et al. 2023. Currently there is no evidence that M. genitalium is a cause of pharyngitis and insufficient evidence that it is a cause of vaginitis, proctitis, or epididymo-orchitis Baiers, et al. 2024; Yazdy, et al. 2023; Manhart, et al. 2022; Read, et al. 2019; Horner and Martin 2017.
Laboratory Testing and Diagnosis
| RECOMMENDATIONS |
Laboratory Testing and Diagnosis
|
Abbreviations: NAAT, nucleic acid amplification testing; PID, pelvic inflammatory disease. |
M. genitalium has no cell wall and can take months to grow in culture; thus, traditional methods of diagnosis with gram stain or culture are not useful. Diagnosis was difficult until NAAT became available. NAAT is the preferred U.S. Food and Drug Administration (FDA)-approved diagnostic method for M. genitalium infection. FDA-approved tests currently cleared for use on urine, vaginal, endocervical, urethra, and penile meatus specimens are the Aptima Mycoplasma Genitalium Assay (Hologic Inc) and Cobas TV/MG Assay (Roche Molecular Systems, Inc.). The latter detects both M. genitalium and Trichomonas vaginalis from a single specimen. For both assays, FDA labeling indicates vaginal specimens are preferred for females and urine specimens are preferred for males. Specimens may be self-collected or clinician collected. The Alinity m STI assay (Abbott Molecular, Inc.) detects M. genitalium, T. vaginalis, Neisseria gonorrhoeae, and Chlamydia trachomatis from a single specimen and is validated for self-collected or clinician-collected vaginal swabs or urine specimens. The cobas® liat CT/NG/MG (Roche Molecular Systems, Inc.) assay, a point-of-care Clinical Laboratory Improvement Amendments of 1988 (CLIA)-waived assay for use by nonlaboratory personnel, was approved in 2025 and detects C. trachomatis, N. gonorrhoeae, and M. genitalium from a clinician- or self-collected vaginal swab or urine specimen.
The specimen and site of optimal sensitivity for testing in transgender individuals with a neopenis or neovagina have not been evaluated.
Screening: Available evidence does not support routine screening for M. genitalium in asymptomatic individuals or in any specific population ASHM 2025; Soni, et al. 2025; Baiers, et al. 2024; Manhart, et al. 2023; Yazdy, et al. 2023; Brehony, et al. 2022; Jensen, et al. 2022; Manhart, et al. 2022; CDC 2021; Golden, et al. 2017; Horner and Martin 2017, and the Centers for Disease Control and Prevention (CDC) recommends against routine screening of asymptomatic individuals CDC 2021. Prevalence estimates of M. genitalium in the general population are low, antimicrobial resistance is increasing, the implications of asymptomatic infection are unknown, and treatment options are limited CDC 2021; Fernández-Huerta, et al. 2020; Baumann, et al. 2018; Golden, et al. 2017; Horner and Martin 2017. Spontaneous clearance of asymptomatic M. genitalium has been described in both men and women and is often cleared with standard treatment for sexually transmitted infection (STI) syndromes when either azithromycin or doxycycline are included in the regimen Berdoyes, et al. 2026; Roy, et al. 2026; Ring, et al. 2022.
At present, there is insufficient evidence regarding pregnancy complications and treatment benefits to recommend for or against screening in asymptomatic pregnant individuals Chen, et al. 2023; Frenzer, et al. 2022; Wiesenfeld and Manhart 2017.
Diagnostic testing: The 2021 CDC STI treatment guidelines specify that M. genitalium testing not be performed in initial testing for presenting STI syndromes of cervicitis or urethritis, and to consider testing in individuals with PID CDC 2021. The recommended use of diagnostic testing for M. genitalium in the United States has been limited to individuals with persistent or recurrent symptoms, because of low rates of detection and because many empiric treatment regimens for STIs include drugs that have activity against M. genitalium and have been demonstrated to clear infection in approximately 56% to 86% of cases Roy, et al. 2026. The standard of care for PID (as recommended by the CDC) includes metronidazole, which has activity against M. genitalium, and its inclusion in PID treatment was demonstrated to reduce M. genitalium in follow-up Wood, et al. 2023; CDC 2021; Wiesenfeld, et al. 2021.
Vaginal symptoms have not been strongly associated with detection of M. genitalium, different from the diagnoses of cervicitis or urethritis, specifically Manhart, et al. 2023; Yazdy, et al. 2023; Brehony, et al. 2022; Latimer, et al. 2022. Diagnoses of persistent, recurrent urethritis in STI clinics have been increasing since 2015, and it is suspected that M. genitalium and other pathogens not identified by routine testing may play a role Llata, et al. 2024. San Francisco City Clinic implemented doxycycline as initial therapy for nongonococcal urethritis (NGU) along with M. genitalium testing at initial visits, and found that this strategy reduced visits for persistent or recurrent NGU from 8% to 3% (P<.0001) Johnson, et al. 2023; however, it is unclear which intervention led to this change, as more than half of infections may be cured by doxycycline alone, and 69% of patients had no microbiologic diagnosis, compared with 82% before intervention.
International guidelines recommend that M. genitalium testing be reserved for symptomatic individuals and ongoing sex partners of individuals who test positive; however, recommendations for timing of testing (e.g., initial for acute symptoms or STI syndromes vs. second-line for persistent/recurrent symptoms) differ ASHM 2025; Soni, et al. 2025; Jensen, et al. 2022; Public Health Agency of Canada 2022.
This evolving body of evidence demonstrates that the optimal timing for diagnostic testing for M. genitalium remains uncertain. This committee suggests limiting M. genitalium testing to circumstances in which STI signs or symptoms persist despite empiric treatment for gonorrhea and chlamydia.
Testing of sex partners: There is little evidence to date to guide the management for sex partners of individuals diagnosed with M. genitalium infection. The CDC and most international guidelines suggest limiting M. genitalium testing and treatment to ongoing sex partners of individuals diagnosed and treated for symptomatic M. genitalium infection (see guideline section Treatment > Partner Treatment for more detail).
| KEY POINT |
|
Resistance testing: Molecular tests that detect both M. genitalium and antibiotic-associated resistance mutations are available. ARUP Laboratories and LabCorp offer macrolide reflex testing approved for use in New York State for NAAT-positive specimens. The association of certain resistance mutations with clinical treatment failure is inconsistent for quinolone antibiotics Yuan, et al. 2025; Conway, et al. 2020, and quinolone resistance assays are not currently available commercially in the United States. However, resistance testing has been demonstrated to be a clinically useful tool to guide treatment, resulting in high cure rates, as evidenced by the resistance-guided antimicrobial therapy model (see guideline section Treatment) Durukan, et al. 2020. To optimally deliver 2-step resistance-guided therapy, diagnostic testing should include reflex to macrolide resistance testing when available.
Treatment
| RECOMMENDATIONS |
Treatment
|
Abbreviation: PID, pelvic inflammatory disease. |
Azithromycin, doxycycline, and moxifloxacin are the most frequently used antibacterial agents for treatment of M. genitalium infection (see Table 1, below). There is geographic variability in cure rates and prevalence of antimicrobial resistance with respect to these antibiotics. Rates of microbiologic cure with use of single-antibiotic regimens in a New York City population, excluding sequential therapy, were 82% with moxifloxacin, 43% with single-dose azithromycin, 31% with a multiday course of azithromycin, and 60% with doxycycline Mullis, et al. 2024. In France, however, the cure rate with single-dose azithromycin was relatively high at 86% (18/21) of cases, and doxycycline cured 55.6% (10/18) Roy, et al. 2026.
Antimicrobial Resistance
In the MyGeniUS study, the prevalence of macrolide resistance-associated mutations among included sexually transmitted infection (STI) clinics across 4 regions in the United States was 59.1%, with values ranging from 51.3% to 70.6% Manhart, et al. 2023. Although not statistically significant, a systematic review examining resistance mutations in M. genitalium globally through 2023 noted an overall downward trend in macrolide resistance mutations to 33.3%, and stable overall prevalence of the primary mutation conferring fluoroquinolone resistance at 14% Chua, et al. 2025. Factors associated with macrolide resistance mutations include male-to-male sexual contact, use of HIV pre-exposure prophylaxis, a recent STI, recurrent bacterial STIs, STI coinfection, and use of antibiotics within the previous 30 days Chua, et al. 2025; Sokoll, et al. 2023; De Baetselier, et al. 2022; Bercot, et al. 2021; Broad, et al. 2021; De Baetselier, et al. 2021; de Salazar, et al. 2021; Latimer, et al. 2020; Li, et al. 2020; Anagrius, et al. 2013.
Several medications have been studied for M. genitalium treatment after initial treatment failure. Minocycline cured 67% to 71% of M. genitalium infections in small observational studies Clarke, et al. 2023; Bachmann, et al. 2020; Doyle, et al. 2020. Metronidazole and tinidazole have activity against M. genitalium, and when metronidazole has been combined with minocycline or doxycycline, cure rates are 80% or higher Htaik, et al. 2025; Wood, et al. 2023; Wiesenfeld, et al. 2021. Monotherapy with nitroimidazoles may also be effective, but evidence is limited to case reports and in vitro data Liscynesky, et al. 2025; Wood, et al. 2023. Newer agents such as omadacycline, zoliflodacin, and gepotidacin have demonstrated activity against M. genitalium in vitro Waites, et al. 2022; Jensen, et al. 2020; Damiao Gouveia, et al. 2018, but no in vivo efficacy data are available. A 2023 case report from the United Kingdom describes successful treatment with chloramphenicol for persistent urethritis with macrolide resistance Goodfellow, et al. 2023. Pristinamycin (of varying dosing strategies) has demonstrated cure rates of approximately 75%, and case reports describe its use in combination with other medications discussed above, but pristinamycin is not available in the United States Raccagni, et al. 2023; Doyle, et al. 2020.
Two-Step Treatment Approach
Updates to treatment recommendations in the United States and elsewhere address the emerging concern of antimicrobial resistance across multiple drug classes. With evidence of increasing macrolide resistance and treatment failures associated with a single dose of azithromycin 1 g, in 2021, the Centers for Disease Control and Prevention (CDC) recommended against use of this regimen in favor of 2-step antibiotic therapy Horner, et al. 2018; Gesink, et al. 2016; Manhart, et al. 2013. Pretreatment with doxycycline has been shown to decrease the overall bacterial burden, making treatment with a second follow-up drug more efficacious Durukan, et al. 2020; Anagrius, et al. 2013; Björnelius, et al. 2008.
Table 1, below, outlines recommended antimicrobial regimens for M. genitalium treatment.
| Abbreviations: FDA, U.S. Food and Drug Administration; NAAT, nucleic acid amplification testing; PID, pelvic inflammatory disease; STI, sexually transmitted infection.
Notes:
|
||
| Table 1: Recommended Antimicrobial Regimens for Mycoplasma genitalium Treatment [a] | ||
| Selected Conditions | Oral Regimens | Considerations |
| Resistance testing unavailable
or Macrolide resistant |
Doxycycline 100 mg twice daily for 7 days
followed by moxifloxacin 400 mg once daily for 7 days |
|
| Macrolide susceptible
or Moxifloxacin unavailable |
Doxycycline 100 mg twice daily for 7 days
followed by azithromycin 1 g on day 1 followed by azithromycin 500 mg once daily for 3 days |
|
The CDC 2021 sexually transmitted infection (STI) Treatment guidelines include treatment recommendations for uncomplicated chlamydial infections, nongonococcal urethritis, and cervicitis with oral doxycycline 100 mg twice daily for 7 days CDC 2021. This facilitates use of a 2-step doxycycline-containing regimen for individuals with persistent or recurrent urethritis or cervicitis who return for follow-up. Standard empiric therapy for PID also includes doxycycline as a component. The CDC recommends that when testing results become available after treatment initiation in cases of PID attributed to M. genitalium, moxifloxacin should be added to the empiric PID regimen rather than given sequentially CDC 2021. For PID related to M. genitalium or the PID clinical syndrome in general, a 14-day course of moxifloxacin was found to be effective Ovens, et al. 2020; Latimer, et al. 2019; Judlin, et al. 2010; Ross, et al. 2006. Because of emerging resistance overall and a lack of treatment alternatives, Australian, Canadian, and European STI guidelines do not recommend moxifloxacin for initial empiric treatment of M. genitalium infection ASHM 2025; Soni, et al. 2025; Jensen, et al. 2022; Public Health Agency of Canada 2022, although, notably, access to antimicrobial resistance testing outside the United States is more widely accessible to guide treatment selection.
Australian and British treatment guidelines also recommend a 2-step treatment approach ASHM 2025; Soni, et al. 2025. In Australia, cure rates reached more than 90% with the implementation of resistance-guided therapy (RGT) Vodstrcil, et al. 2022; Durukan, et al. 2020: Individuals with an STI syndrome received 7 days of oral doxycycline 100 mg twice daily empirically and then, if found to have M. genitalium infection without macrolide resistance, received 2.5 g oral azithromycin over 4 days (1 g on day 1 and 500 mg once daily on days 2 through 4). After initial treatment with doxycycline, individuals with macrolide-resistant M. genitalium infection received oral moxifloxacin 400 mg once daily for 7 days. A test of cure was performed 2 to 4 weeks after treatment. The cure rate with the RGT approach was 92%, even in regions with reported quinolone resistance of 15% to 20% Durukan, et al. 2020. Use of doxycycline followed by moxifloxacin or sitafloxacin (not available in the United States) continued to result in high cure rates Yuan, et al. 2025; Vodstrcil, et al. 2022.
Treating asymptomatic M. genitalium infection: Asymptomatic M. genitalium infection is common, and the benefit of treating asymptomatic individuals has not been clearly demonstrated. There is a theoretical benefit to treating asymptomatic ongoing partners of individuals with symptomatic infection (see Partner Treatment, below); treatment of asymptomatic M. genitalium is otherwise not recommended.
Test of cure: The timeframe used for test of cure in the published literature is highly variable. Testing too soon after treatment carries the risk of detecting residual noninfectious particles. The CDC recommends a test of cure at 21 days for those treated with the 2-step doxycycline plus azithromycin regimen (see Table 1, above) who did not complete macrolide resistance testing CDC 2021. This committee prefers that test of cure be reserved for patients who remain symptomatic and obtained no sooner than 21 days after treatment.
STI coinfection: When coinfection with another STI is present, it remains unclear based on available evidence whether M. genitalium is a true pathogen requiring treatment. If M. genitalium is detected in a patient with another STI, this committee recommends reserving treatment for M. genitalium for those with persistent symptoms despite appropriate treatment of the other infection (e.g., gonorrhea, chlamydia, trichomoniasis).
Managing Treatment Failure
It is important to distinguish between reinfection and treatment failure; see Partner Treatment, below. To aid in management of M. genitalium infection, macrolide resistance testing (if not already performed at diagnosis) should be obtained to help guide antimicrobial regimen selection going forward. For individuals with persistent infection despite treatment with recommended 2-step therapy, minocycline 100 mg orally twice daily for 14 days is an option supported by observational data Clarke, et al. 2023; Doyle, et al. 2020. If this regimen is unsuccessful, nitroimidazoles may be considered, although optimal drug choice and dosing vary. In cases of treatment failure across multiple drug classes and detected macrolide resistance, treatment options with case reports of success include the following: 1) minocycline 100 mg orally twice daily combined with metronidazole 500 mg orally twice daily for 14 days (tinidazole 2 g orally once daily may be substituted for the twice daily metronidazole), and 2) tinidazole 2 g orally once daily for 7 days Htaik, et al. 2025; Liscynesky, et al. 2025; Wood, et al. 2023.
| KEY POINT |
|
Pregnancy
Moxifloxacin and doxycycline are generally not recommended for pregnant individuals. An azithromycin-only course of treatment (e.g., azithromycin 1 g on day 1 followed by 500 mg once daily on days 2, 3, and 4) can be considered with acknowledgment of the risk of treatment failure (see discussion above). Given the high rates of azithromycin resistance, shared decision-making is warranted after considering the potential risks of untreated M. genitalium infection during pregnancy and the potential risk of adverse drug events associated with antibiotics not generally used during pregnancy. Some individuals may elect to postpone treatment until after delivery, depending on individual circumstances Jensen, et al. 2022. International guidelines advise caution when selecting treatment for pregnant individuals, generally proposing initial treatment with azithromycin monotherapy (with varying dosing strategies), with some suggesting pristinamycin (not available in the United States) as an alternative and acknowledging its limited safety data Drew and Eogan 2024.
Some studies have raised concerns about associations between M. genitalium infection and infertility and pregnancy complications, although the evidence is limited and insufficient to demonstrate causation. A meta-analysis of available studies suggested significant associations with preterm birth and spontaneous abortion Lis, et al. 2015. In this same analysis, the risk of infertility was described as elevated but was not statistically significant Lis, et al. 2015. A systematic review that examined multiple mycoplasma species and spontaneous abortion, specifically, found that the presence of M. genitalium (as detected by polymerase chain reaction [PCR] test) was not associated with spontaneous abortion Chen, et al. 2023. Some studies have reported associations between M. genitalium infection and preterm birth and low birth weight, but the lack of control for confounding within these studies limit the strength of the analyses Scoullar, et al. 2024; Frenzer, et al. 2022. Much of the existing data are from observational studies and are further limited by confounding and use of serology before 2019 Frenzer, et al. 2022.
Partner Treatment
There is insufficient evidence to determine whether sex partners of individuals with symptomatic M. genitalium infection should receive treatment only if infection is detected through a laboratory test ASHM 2025; Soni, et al. 2025; Jensen, et al. 2022; Public Health Agency of Canada 2022 or regardless of test results. In alignment with CDC guidelines, to prevent potential reinfection of the index patient, this committee recommends offering testing to ongoing sex partners and limiting treatment to those with positive test results. Partners can be treated with the same regimen as the index patient CDC 2021.
All Recommendations
| ALL RECOMMENDATIONS: MYCOPLASMA GENITALIUM MANAGEMENT IN ADULTS |
Laboratory Testing and Diagnosis
Treatment
|
Abbreviations: NAAT, nucleic acid amplification testing; PID, pelvic inflammatory disease. |
Shared Decision-Making
Download Printable PDF of Shared Decision-Making Statement
Date of current publication: August 8, 2023
Lead authors: Jessica Rodrigues, MS; Jessica M. Atrio, MD, MSc; and Johanna L. Gribble, MA
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: August 8, 2023
Rationale
Throughout its guidelines, the New York State Department of Health (NYSDOH) AIDS Institute (AI) Clinical Guidelines Program recommends “shared decision-making,” an individualized process central to patient-centered care. With shared decision-making, clinicians and patients engage in meaningful dialogue to arrive at an informed, collaborative decision about a patient’s health, care, and treatment planning. The approach to shared decision-making described here applies to recommendations included in all program guidelines. The included elements are drawn from a comprehensive review of multiple sources and similar attempts to define shared decision-making, including the Institute of Medicine’s original description [Institute of Medicine 2001]. For more information, a variety of informative resources and suggested readings are included at the end of the discussion.
Benefits
The benefits to patients that have been associated with a shared decision-making approach include:
- Decreased anxiety [Niburski, et al. 2020; Stalnikowicz and Brezis 2020]
- Increased trust in clinicians [Acree, et al. 2020; Groot, et al. 2020; Stalnikowicz and Brezis 2020]
- Improved engagement in preventive care [McNulty, et al. 2022; Scalia, et al. 2022; Bertakis and Azari 2011]
- Improved treatment adherence, clinical outcomes, and satisfaction with care [Crawford, et al. 2021; Bertakis and Azari 2011; Robinson, et al. 2008]
- Increased knowledge, confidence, empowerment, and self-efficacy [Chen, et al. 2021; Coronado-Vázquez, et al. 2020; Niburski, et al. 2020]
Approach
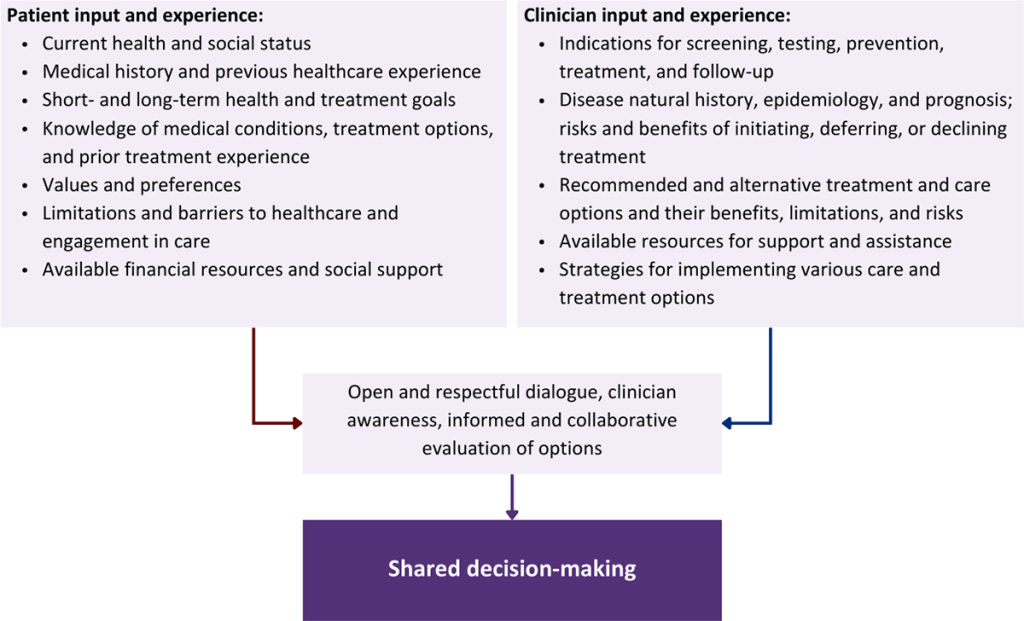
Collaborative care: Shared decision-making is an approach to healthcare delivery that respects a patient’s autonomy in responding to a clinician’s recommendations and facilitates dynamic, personalized, and collaborative care. Through this process, a clinician engages a patient in an open and respectful dialogue to elicit the patient’s knowledge, experience, healthcare goals, daily routine, lifestyle, support system, cultural and personal identity, and attitudes toward behavior, treatment, and risk. With this information and the clinician’s clinical expertise, the patient and clinician can collaborate to identify, evaluate, and choose from among available healthcare options [Coulter and Collins 2011]. This process emphasizes the importance of a patient’s values, preferences, needs, social context, and lived experience in evaluating the known benefits, risks, and limitations of a clinician’s recommendations for screening, prevention, treatment, and follow-up. As a result, shared decision-making also respects a patient’s autonomy, agency, and capacity in defining and managing their healthcare goals. Building a clinician-patient relationship rooted in shared decision-making can help clinicians engage in productive discussions with patients whose decisions may not align with optimal health outcomes. Fostering open and honest dialogue to understand a patient’s motivations while suspending judgment to reduce harm and explore alternatives is particularly vital when a patient chooses to engage in practices that may exacerbate or complicate health conditions [Halperin, et al. 2007].
Options: Implicit in the shared decision-making process is the recognition that the “right” healthcare decisions are those made by informed patients and clinicians working toward patient-centered and defined healthcare goals. When multiple options are available, shared decision-making encourages thoughtful discussion of the potential benefits and potential harms of all options, which may include doing nothing or waiting. This approach also acknowledges that efficacy may not be the most important factor in a patient’s preferences and choices [Sewell, et al. 2021].
Clinician awareness: The collaborative process of shared decision-making is enhanced by a clinician’s ability to demonstrate empathic interest in the patient, avoid stigmatizing language, employ cultural humility, recognize systemic barriers to equitable outcomes, and practice strategies of self-awareness and mitigation against implicit personal biases [Parish, et al. 2019].
Caveats: It is important for clinicians to recognize and be sensitive to the inherent power and influence they maintain throughout their interactions with patients. A clinician’s identity and community affiliations may influence their ability to navigate the shared decision-making process and develop a therapeutic alliance with the patient and may affect the treatment plan [KFF 2023; Greenwood, et al. 2020]. Furthermore, institutional policy and regional legislation, such as requirements for parental consent for gender-affirming care for transgender people or insurance coverage for sexual health care, may infringe upon a patient’s ability to access preventive- or treatment-related care [Sewell, et al. 2021].
Figure 1: Elements of Shared Decision-Making
Health equity: Adapting a shared decision-making approach that supports diverse populations is necessary to achieve more equitable and inclusive health outcomes [Castaneda-Guarderas, et al. 2016]. For instance, clinicians may need to incorporate cultural- and community-specific considerations into discussions with women, gender-diverse individuals, and young people concerning their sexual behaviors, fertility intentions, and pregnancy or lactation status. Shared decision-making offers an opportunity to build trust among marginalized and disenfranchised communities by validating their symptoms, values, and lived experience. Furthermore, it can allow for improved consistency in patient screening and assessment of prevention options and treatment plans, which can reduce the influence of social constructs and implicit bias [Castaneda-Guarderas, et al. 2016].
Clinician bias has been associated with health disparities and can have profoundly negative effects [FitzGerald and Hurst 2017; Hall, et al. 2015]. It is often challenging for clinicians to recognize and set aside personal biases and to address biases with peers and colleagues. Consciously or unconsciously, negative or stigmatizing assumptions are often made about patient characteristics, such as race, ethnicity, gender, sexual orientation, mental health, and substance use [Avery, et al. 2019; van Boekel, et al. 2013; Livingston, et al. 2012]. With its emphasis on eliciting patient information, a shared decision-making approach encourages clinicians to inquire about patients’ lived experiences rather than making assumptions and to recognize the influence of that experience in healthcare decision-making.
Stigma: Stigma may prevent individuals from seeking or receiving treatment and harm reduction services [Tsai, et al. 2019]. Among people with HIV, stigma and medical mistrust remain significant barriers to healthcare utilization, HIV diagnosis, and medication adherence and can affect disease outcomes [Turan, et al. 2017; Chambers, et al. 2015], and stigma among clinicians against people who use substances has been well-documented [Stone, et al. 2021; Tsai, et al. 2019; van Boekel, et al. 2013]. Sexual and reproductive health, including strategies to prevent HIV transmission, acquisition, and progression, may be subject to stigma, bias, social influence, and violence.
| SHARED DECISION-MAKING IN HIV CARE |
|
Resources and Suggested Reading
In addition to the references cited below, the following resources and suggested reading may be useful to clinicians.
| RESOURCES |
References
Acree ME, McNulty M, Blocker O, et al. Shared decision-making around anal cancer screening among black bisexual and gay men in the USA. Cult Health Sex 2020;22(2):201-16. [PMID: 30931831]
Avery JD, Taylor KE, Kast KA, et al. Attitudes toward individuals with mental illness and substance use disorders among resident physicians. Prim Care Companion CNS Disord 2019;21(1):18m02382. [PMID: 30620451]
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med 2011;24(3):229-39. [PMID: 21551394]
Castaneda-Guarderas A, Glassberg J, Grudzen CR, et al. Shared decision making with vulnerable populations in the emergency department. Acad Emerg Med 2016;23(12):1410-16. [PMID: 27860022]
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health 2015;15:848. [PMID: 26334626]
Chen CH, Kang YN, Chiu PY, et al. Effectiveness of shared decision-making intervention in patients with lumbar degenerative diseases: a randomized controlled trial. Patient Educ Couns 2021;104(10):2498-2504. [PMID: 33741234]
Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, et al. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore) 2020;99(32):e21389. [PMID: 32769870]
Coulter A, Collins A. Making shared decision-making a reality: no decision about me, without me. 2011. https://www.kingsfund.org.uk/sites/default/files/Making-shared-decision-making-a-reality-paper-Angela-Coulter-Alf-Collins-July-2011_0.pdf
Crawford J, Petrie K, Harvey SB. Shared decision-making and the implementation of treatment recommendations for depression. Patient Educ Couns 2021;104(8):2119-21. [PMID: 33563500]
FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics 2017;18(1):19. [PMID: 28249596]
Greenwood BN, Hardeman RR, Huang L, et al. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020;117(35):21194-21200. [PMID: 32817561]
Groot G, Waldron T, Barreno L, et al. Trust and world view in shared decision making with indigenous patients: a realist synthesis. J Eval Clin Pract 2020;26(2):503-14. [PMID: 31750600]
Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health 2015;105(12):e60-76. [PMID: 26469668]
Halperin B, Melnychuk R, Downie J, et al. When is it permissible to dismiss a family who refuses vaccines? Legal, ethical and public health perspectives. Paediatr Child Health 2007;12(10):843-45. [PMID: 19043497]
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. 2001. https://www.ncbi.nlm.nih.gov/books/NBK222274/
KFF. Key data on health and health care by race and ethnicity. 2023 Mar 15. https://www.kff.org/racial-equity-and-health-policy/report/key-data-on-health-and-health-care-by-race-and-ethnicity/ [accessed 2023 May 19]
Livingston JD, Milne T, Fang ML, et al. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction 2012;107(1):39-50. [PMID: 21815959]
McNulty MC, Acree ME, Kerman J, et al. Shared decision making for HIV pre-exposure prophylaxis (PrEP) with black transgender women. Cult Health Sex 2022;24(8):1033-46. [PMID: 33983866]
Niburski K, Guadagno E, Abbasgholizadeh-Rahimi S, et al. Shared decision making in surgery: a meta-analysis of existing literature. Patient 2020;13(6):667-81. [PMID: 32880820]
Parish SJ, Hahn SR, Goldstein SW, et al. The International Society for the Study of Women’s Sexual Health process of care for the identification of sexual concerns and problems in women. Mayo Clin Proc 2019;94(5):842-56. [PMID: 30954288]
Robinson JH, Callister LC, Berry JA, et al. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008;20(12):600-607. [PMID: 19120591]
Scalia P, Durand MA, Elwyn G. Shared decision-making interventions: an overview and a meta-analysis of their impact on vaccine uptake. J Intern Med 2022;291(4):408-25. [PMID: 34700363]
Sewell WC, Solleveld P, Seidman D, et al. Patient-led decision-making for HIV preexposure prophylaxis. Curr HIV/AIDS Rep 2021;18(1):48-56. [PMID: 33417201]
Stalnikowicz R, Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract 2020;26(2):431-38. [PMID: 31989727]
Stone EM, Kennedy-Hendricks A, Barry CL, et al. The role of stigma in U.S. primary care physicians’ treatment of opioid use disorder. Drug Alcohol Depend 2021;221:108627. [PMID: 33621805]
Tsai AC, Kiang MV, Barnett ML, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med 2019;16(11):e1002969. [PMID: 31770387]
Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav 2017;21(1):283-91. [PMID: 27272742]
van Boekel LC, Brouwers EP, van Weeghel J, et al. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013;131(1-2):23-35. [PMID: 23490450]
References
Anagrius C., Loré B., Jensen J. S. Treatment of Mycoplasma genitalium. Observations from a Swedish STD clinic. PLoS One 2013;8(4):e61481. [PMID: 23593483]
ASHM. Australian STI management guidelines for use in primary care: Mycoplasma genitalium. 2025 Sep. https://sti.guidelines.org.au/sexually-transmissible-infections/mycoplasma-genitalium/ [accessed 2026 Feb 25]
Bachmann L. H., Kirkcaldy R. D., Geisler W. M., et al. Prevalence of Mycoplasma genitalium infection, antimicrobial resistance mutations, and symptom resolution following treatment of urethritis. Clin Infect Dis 2020;71(10):e624-32. [PMID: 32185385]
Baiers R. A., Ryan D. T., Clifford A., et al. Asymptomatic rectal bacterial pathogens show large prospective relationships with HIV incidence in a cohort of young sexual and gender minorities: implications for STI screening and HIV prevention. Open Forum Infect Dis 2024;11(8):ofae444. [PMID: 39183815]
Baumann L., Cina M., Egli-Gany D., et al. Prevalence of Mycoplasma genitalium in different population groups: systematic review and meta-analysis. Sex Transm Infect 2018;94(4):255-62. [PMID: 29440466]
Bercot B., Charreau I., Rousseau C., et al. High prevalence and high rate of antibiotic resistance of Mycoplasma genitalium infections in men who have sex with men: a substudy of the ANRS IPERGAY pre-exposure prophylaxis trial. Clin Infect Dis 2021;73(7):e2127-33. [PMID: 33305785]
Berdoyes M., Bebear C., Roy C. L., et al. Spontaneous clearance of vaginal Mycoplasma genitalium in women undergoing pregnancy termination: a prospective cohort study. BJOG 2026;133(5):1074-82. [PMID: 41502158]
Björnelius E., Anagrius C., Bojs G., et al. Antibiotic treatment of symptomatic Mycoplasma genitalium infection in Scandinavia: a controlled clinical trial. Sex Transm Infect 2008;84(1):72-76. [PMID: 17932127]
Brehony C., Eogan M., Lambert J. S., et al. Evaluation of molecular testing for Mycoplasma genitalium for symptomatic women. Ir J Med Sci 2022;191(4):1771-75. [PMID: 34546502]
Broad C. E., Furegato M., Harrison M. A., et al. High prevalence of coinfection of azithromycin-resistant Mycoplasma genitalium with other STIs: a prospective observational study of London-based symptomatic and STI-contact clinic attendees. Sex Transm Infect 2021;97(1):63-68. [PMID: 32393529]
Calas A., Zemali N., Camuset G., et al. Prevalence of urogenital, anal, and pharyngeal infections with Chlamydia trachomatis, Neisseria gonorrhoeae, and Mycoplasma genitalium: a cross-sectional study in Reunion island. BMC Infect Dis 2021;21(1):95. [PMID: 33478403]
CDC. Sexually transmitted infections treatment guidelines, 2021: Mycoplasma genitalium. 2021 Jul 22. https://www.cdc.gov/std/treatment-guidelines/mycoplasmagenitalium.htm [accessed 2026 Feb 25]
Chen W., Xiong S., Shen X., et al. The association between genital mycoplasma infection and spontaneous abortion: A systematic review and meta-analysis. Reprod Toxicol 2023;116:108334. [PMID: 36608834]
Chua T. P., Vodstrcil L. A., Murray G. L., et al. Evolving patterns of macrolide and fluoroquinolone resistance in Mycoplasma genitalium: an updated systematic review and meta-analysis. Lancet Microbe 2025;6(7):101047. [PMID: 40147462]
Clarke E. J., Vodstrcil L. A., Plummer E. L., et al. Efficacy of minocycline for the treatment of Mycoplasma genitalium. Open Forum Infect Dis 2023;10(8):ofad427. [PMID: 37608915]
Conway R. J., Cook S., Malone C., et al. Clearance of Mycoplasma genitalium infection with moxifloxacin in the presence of quinolone resistance-associated mutations. Sex Transm Dis 2020;47(3):197-98. [PMID: 31738298]
Damiao Gouveia A. C., Unemo M., Jensen J. S. In vitro activity of zoliflodacin (ETX0914) against macrolide-resistant, fluoroquinolone-resistant and antimicrobial-susceptible Mycoplasma genitalium strains. J Antimicrob Chemother 2018;73(5):1291-94. [PMID: 29444242]
De Baetselier I., Kenyon C., Vanden Berghe W., et al. An alarming high prevalence of resistance-associated mutations to macrolides and fluoroquinolones in Mycoplasma genitalium in Belgium: results from samples collected between 2015 and 2018. Sex Transm Infect 2021;97(4):297-303. [PMID: 32769204]
De Baetselier I., Vuylsteke B., Reyniers T., et al. Worryingly high prevalence of resistance-associated mutations to macrolides and fluoroquinolones in Mycoplasma genitalium among men who have sex with men with recurrent sexually transmitted infections. Int J STD AIDS 2022;33(4):385-90. [PMID: 35094623]
de Salazar A., Barrientos-Durán A., Espadafor B., et al. Macrolide and fluoroquinolone resistance of Mycoplasma genitalium in southern Spain, 2018-2019. Sex Transm Infect 2021;97(1):8-10. [PMID: 32661071]
Dehon P. M., Hagensee M. E., Sutton K. J., et al. Histological evidence of chronic Mycoplasma genitalium-induced cervicitis in HIV-infected women: a retrospective cohort study. J Infect Dis 2016;213(11):1828-35. [PMID: 26783349]
Doyle M., Vodstrcil L. A., Plummer E. L., et al. Nonquinolone options for the treatment of Mycoplasma genitalium in the era of increased resistance. Open Forum Infect Dis 2020;7(8):ofaa291. [PMID: 32782911]
Drew R. J., Eogan M. Treatment of Mycoplasma genitalium infection in pregnancy: A systematic review of international guidelines. Int J Gynaecol Obstet 2024;166(1):27-34. [PMID: 38491782]
Durukan D., Read T. R. H., Murray G., et al. Resistance-guided antimicrobial therapy using doxycycline-moxifloxacin and doxycycline-2.5 g azithromycin for the treatment of Mycoplasma genitalium infection: efficacy and tolerability. Clin Infect Dis 2020;71(6):1461-68. [PMID: 31629365]
Fernández-Huerta M., Barberá M. J., Esperalba J., et al. Prevalence of Mycoplasma genitalium and macrolide resistance among asymptomatic people visiting a point of care service for rapid STI screening: a cross-sectional study. Sex Transm Infect 2020;96(4):300-305. [PMID: 31451540]
Frenzer C., Egli-Gany D., Vallely L. M., et al. Adverse pregnancy and perinatal outcomes associated with Mycoplasma genitalium: systematic review and meta-analysis. Sex Transm Infect 2022;98(3):222-27. [PMID: 35351816]
Gaydos C., Maldeis N. E., Hardick A., et al. Mycoplasma genitalium as a contributor to the multiple etiologies of cervicitis in women attending sexually transmitted disease clinics. Sex Transm Dis 2009;36(10):598-606. [PMID: 19704398]
Gaydos C. A., Manhart L. E., Taylor S. N., et al. Molecular testing for mycoplasma genitalium in the united states: Results from the AMES prospective multicenter clinical study. J Clin Microbiol 2019;57(11):e01125-19. [PMID: 31484702]
Gesink D., Racey C. S., Seah C., et al. Mycoplasma genitalium in Toronto, Ont: estimates of prevalence and macrolide resistance. Can Fam Physician 2016;62(2):e96-101. [PMID: 27331225]
Golden M. R., Workowski K. A., Bolan G. Developing a public health response to Mycoplasma genitalium. J Infect Dis 2017;216(Suppl 2):S420-26. [PMID: 28838079]
Goodfellow J. J., Hughes S., Smith J., et al. Novel use of oral chloramphenicol for treatment-resistant Mycoplasma genitalium. Sex Transm Infect 2023;99(3):208-10. [PMID: 36717253]
Horner P., Ingle S. M., Garrett F., et al. Which azithromycin regimen should be used for treating Mycoplasma genitalium? A meta-analysis. Sex Transm Infect 2018;94(1):14-20. [PMID: 28717050]
Horner P., Martin D. H. Mycoplasma genitalium infection in men. J Infect Dis 2017;216(Suppl 2):S396-405. [PMID: 28838074]
Htaik K., Vodstrcil L. A., Plummer E. L., et al. Efficacy and tolerability of the combination of minocycline and metronidazole for macrolide-resistant Mycoplasma genitalium. J Antimicrob Chemother 2025;80(7):1878-84. [PMID: 40401482]
Htaik K., Vodstrcil L. A., Plummer E. L., et al. Systematic review and meta-analysis of the association between Mycoplasma genitalium and Pelvic inflammatory disease (PID). Clin Infect Dis 2024;82(2):e371-79. [PMID: 38845565]
Huppert J. S., Mortensen J. E., Reed J. L., et al. Mycoplasma genitalium detected by transcription-mediated amplification is associated with Chlamydia trachomatis in adolescent women. Sex Transm Dis 2008;35(3):250-54. [PMID: 18490867]
Jensen J. S., Cusini M., Gomberg M., et al. 2021 European guideline on the management of Mycoplasma genitalium infections. J Eur Acad Dermatol Venereol 2022;36(5):641-50. [PMID: 35182080]
Jensen J. S., Norgaard C., Scangarella-Oman N., et al. In vitro activity of the first-in-class triazaacenaphthylene gepotidacin alone and in combination with doxycycline against drug-resistant and -susceptible Mycoplasma genitalium. Emerg Microbes Infect 2020;9(1):1388-92. [PMID: 32552547]
Johnson K. A., Sankaran M., Kohn R. P., et al. Testing for Mycoplasma genitalium and using doxycycline as first-line therapy at initial presentations for non-gonococcal urethritis (NGU) correlate with reductions in persistent NGU. Clin Infect Dis 2023;76(9):1674-77. [PMID: 36575605]
Judlin P., Liao Q., Liu Z., et al. Efficacy and safety of moxifloxacin in uncomplicated pelvic inflammatory disease: the MONALISA study. BJOG 2010;117(12):1475-84. [PMID: 20716255]
Latimer R., Read T. R., Vodstrcil L. A., et al. Clinical features and therapeutic response in women meeting criteria for presumptive treatment for pelvic inflammatory disease associated with Mycoplasma genitalium. Sex Transm Dis 2019;46(2):73-79. [PMID: 30640861]
Latimer R. L., Vodstrcil L., De Petra V., et al. Extragenital Mycoplasma genitalium infections among men who have sex with men. Sex Transm Infect 2020;96(1):10-18. [PMID: 31217322]
Latimer R. L., Vodstrcil L. A., Plummer E. L., et al. The clinical indications for testing women for Mycoplasma genitalium. Sex Transm Infect 2022;98(4):277-85. [PMID: 34210839]
Li Y., Su X., Le W., et al. Mycoplasma genitalium in symptomatic male urethritis: Macrolide use is associated with increased resistance. Clin Infect Dis 2020;70(5):805-10. [PMID: 30972419]
Lis R., Rowhani-Rahbar A., Manhart L. E. Mycoplasma genitalium infection and female reproductive tract disease: a meta-analysis. Clin Infect Dis 2015;61(3):418-26. [PMID: 25900174]
Liscynesky C., Lipps A., Bazan J. A. Successful treatment of Mycoplasma genitalium urethritis with high-dose tinidazole. Sex Transm Dis 2025;52(2):e2-4. [PMID: 39774093]
Llata E., Tromble E., Schumacher C., et al. Should we be testing for Mycoplasma genitalium on initial presentation? trends in persistent/recurrent urethritis among men presenting for care in STD clinics, 2015-2019, STD Surveillance Network. Sex Transm Dis 2024;51(7):493-98. [PMID: 38602771]
Lusk M. J., Konecny P., Naing Z. W., et al. Mycoplasma genitalium is associated with cervicitis and HIV infection in an urban Australian STI clinic population. Sex Transm Infect 2011;87(2):107-9. [PMID: 21071566]
Manhart L. E., Geisler W. M., Bradshaw C. S., et al. Weighing potential benefits and harms of Mycoplasma genitalium testing and treatment approaches. Emerg Infect Dis 2022;28(8):e220094. [PMID: 35876565]
Manhart L. E., Gillespie C. W., Lowens M. S., et al. Standard treatment regimens for nongonococcal urethritis have similar but declining cure rates: a randomized controlled trial. Clin Infect Dis 2013;56(7):934-42. [PMID: 23223595]
Manhart L. E., Holmes K. K., Hughes J. P., et al. Mycoplasma genitalium among young adults in the United States: an emerging sexually transmitted infection. Am J Public Health 2007;97(6):1118-25. [PMID: 17463380]
Manhart L. E., Leipertz G., Soge O. O., et al. Mycoplasma genitalium in the US (MyGeniUS): surveillance data from sexual health clinics in 4 US regions. Clin Infect Dis 2023;77(10):1449-59. [PMID: 37402645]
Mena L., Wang X., Mroczkowski T. F., et al. Mycoplasma genitalium infections in asymptomatic men and men with urethritis attending a sexually transmitted diseases clinic in New Orleans. Clin Infect Dis 2002;35(10):1167-73. [PMID: 12410476]
Menezes M. E., Silver E. J., Goldstein D. Y., et al. Prevalence and factors associated with Mycoplasma genitalium infection in at-risk female adolescents in Bronx County, New York. Sex Transm Dis 2023;50(10):635-41. [PMID: 37255234]
Mitchell C. M., Anyalechi G. E., Cohen C. R., et al. Etiology and diagnosis of pelvic inflammatory disease: looking beyond gonorrhea and chlamydia. J Infect Dis 2021;224(12 Suppl 2):S29-35. [PMID: 34396407]
Mullis C. E., Marlow K. A., Maity A., et al. Clinical presentations and treatment outcomes of Mycoplasma genitalium infections at a large New York City health care system. Sex Transm Dis 2024;51(3):199-205. [PMID: 38100794]
Ovens K. J., Reynolds-Wright J. J., Cross E. L., et al. High rates of treatment failure for Mycoplasma genitalium among men and women attending a sexual health clinic. BMJ Sex Reprod Health 2020;46(2):132-38. [PMID: 31722934]
Public Health Agency of Canada. Mycoplasma genitalium guide: screening and diagnostic testing. 2022 Jul 7. https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/mycoplasma-genitalium/screening-diagnostic-testing.html [accessed 2026 Feb 25]
Raccagni A. R., Bruzzesi E., Spagnuolo V., et al. 'Multidrug-resistant Mycoplasma genitalium urethritis: successful eradication with sequential therapy. Sex Transm Infect 2023;99(1):77. [PMID: 36601744]
Read T. R. H., Murray G. L., Danielewski J. A., et al. Symptoms, sites, and significance of mycoplasma genitalium in men who have sex with men. Emerg Infect Dis 2019;25(4):719-27. [PMID: 30882306]
Ring A., Balakrishna S., Imkamp F., et al. High rates of asymptomatic Mycoplasma genitalium infections with high proportion of genotypic resistance to first-line macrolide treatment among men who have sex with men enrolled in the zurich primary HIV infection study. Open Forum Infect Dis 2022;9(6):ofac217. [PMID: 35783686]
Ross J. D., Cronjé H. S., Paszkowski T., et al. Moxifloxacin versus ofloxacin plus metronidazole in uncomplicated pelvic inflammatory disease: results of a multicentre, double blind, randomised trial. Sex Transm Infect 2006;82(6):446-51. [PMID: 16723364]
Roy C. L., Ferron A., Balcon C., et al. Impact of Chlamydia trachomatis treatment with azithromycin or doxycycline on Mycoplasma genitalium in women. Int J Infect Dis 2026;165:108404. [PMID: 41570889]
Schwebke J. R., Nyirjesy P., Dsouza M., et al. Vaginitis and risk of sexually transmitted infections: results of a multi-center U.S. clinical study using STI nucleic acid amplification testing. J Clin Microbiol 2024;62(9):e0081624. [PMID: 39140739]
Scoullar M. J. L., Melepia P., Peach E., et al. Mycoplasma genitalium in pregnancy, including specific co-infections, is associated with lower birthweight: A prospective cohort study. Med 2024;5(9):1123-36.e3. [PMID: 38870930]
Sokoll P. R., Migliavaca C. B., Siebert U., et al. Prevalence of Mycoplasma genitalium infection among HIV PrEP users: a systematic review and meta-analysis. Sex Transm Infect 2023;99(5):351-59. [PMID: 36759179]
Soni S., Fifer H., Al-Shakarchi Y., et al. British Association of Sexual Health and HIV National guideline for the management of infection with Mycoplasma genitalium, 2025. Int J STD AIDS 2025. [PMID: 40673484]
Totten P. A., Schwartz M. A., Sjöström K. E., et al. Association of Mycoplasma genitalium with nongonococcal urethritis in heterosexual men. J Infect Dis 2001;183(2):269-76. [PMID: 11120932]
Vodstrcil L. A., Plummer E. L., Doyle M., et al. Combination therapy for Mycoplasma genitalium, and new insights into the utility of parC mutant detection to improve cure. Clin Infect Dis 2022;75(5):813-23. [PMID: 34984438]
Waites K. B., Crabb D. M., Atkinson T. P., et al. Omadacycline is highly active in vitro against Mycoplasma genitalium. Microbiol Spectr 2022;10(6):e0365422. [PMID: 36314935]
Wiesenfeld H. C., Manhart L. E. Mycoplasma genitalium in women: current knowledge and research priorities for this recently emerged pathogen. J Infect Dis 2017;216(Suppl 2):S389-95. [PMID: 28838078]
Wiesenfeld H. C., Meyn L. A., Darville T., et al. A randomized controlled trial of ceftriaxone and doxycycline, with or without metronidazole, for the treatment of acute pelvic inflammatory disease. Clin Infect Dis 2021;72(7):1181-89. [PMID: 32052831]
Wikström A., Jensen J. S. Mycoplasma genitalium: a common cause of persistent urethritis among men treated with doxycycline. Sex Transm Infect 2006;82(4):276-79. [PMID: 16877573]
Wood G. E., Bradshaw C. S., Manhart L. E. Update in epidemiology and management of Mycoplasma genitalium infections. Infect Dis Clin North Am 2023;37(2):311-33. [PMID: 37105645]
Yazdy G. M., Van Gerwen O. T., Ghanem K. G., et al. Testing for Mycoplasma genitalium in women with vaginal symptoms should not be performed routinely. Sex Transm Dis 2023;50(10):e22-25. [PMID: 37432989]
Yuan M., Le W., Zhao Y., et al. Efficacy of doxycycline-sitafloxacin sequential therapy for urogenital Mycoplasma genitalium infection in Nanjing, China. Sex Transm Dis 2025;52(4):259-65. [PMID: 40053328]
Zhang R., Chung S. L., Lee S. S., et al. Prevalence and resistance patterns of Mycoplasma genitalium infection in people with HIV: a systematic review and meta-analysis. AIDS 2025;39(11):1598-1609. [PMID: 40265621]
Updates, Authorship, and Related Guidelines
| Updates, Authorship, and Related Guidelines | |
| Date of original publication | September 28, 2020 |
| Date of current publication | June 10, 2026 |
| Highlights of changes, additions, and updates in the June 10, 2026 edition |
|
| Intended users | Clinicians who manage sexually transmitted infections in adults aged 18 years and older |
| Lead author |
Daniela E. DiMarco, MD, MPH |
| Writing group |
Rona Vail, MD, AAHIVS; Sanjiv S. Shah, MD, MPH, AAHIVS; Steven M. Fine, MD, PhD; Joseph P. McGowan, MD, FACP, FIDSA, AAHIVS; Samuel T. Merrick, MD, FIDSA; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Anne K. Monroe, MD, MSPH; Marguerite A. Urban, MD; Jessica Rodrigues, MPH, MS; Christopher J. Hoffmann, MD, MPH, MSc, FACP; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD |
| Author and writing group conflict of interest disclosures | There are no author or writing group conflict of interest disclosures. |
| Committee | |
| Developer and funder |
New York State Department of Health AIDS Institute (NYSDOH AI) |
| Development process |
See Guideline Development and Recommendation Ratings Scheme, below. |
| Related NYSDOH AI guidelines |
GuidancePodcast |
Guideline Development and Recommendation Ratings
| Guideline Development: New York State Department of Health AIDS Institute Clinical Guidelines Program | |
| Program manager | Clinical Guidelines Program, Johns Hopkins University School of Medicine, Division of Infectious Diseases. See Program Leadership and Staff. |
| Mission | To produce and disseminate evidence-based, state-of-the-art clinical practice guidelines that establish uniform standards of care for practitioners who provide prevention or treatment of HIV, viral hepatitis, other sexually transmitted infections, and substance use disorders for adults throughout New York State in the wide array of settings in which those services are delivered. |
| Expert committees | The NYSDOH AI Medical Director invites and appoints committees of clinical and public health experts from throughout New York State to ensure that the guidelines are practical, immediately applicable, and meet the needs of care providers and stakeholders in all major regions of New York State, all relevant clinical practice settings, key New York State agencies, and community service organizations. |
| Committee structure |
|
| Disclosure and management of conflicts of interest |
|
| Evidence collection and review |
|
| Recommendation development |
|
| Review and approval process |
|
| External reviews |
|
| Update process |
|
| Recommendation Ratings Scheme | |||
| Strength | Quality of Evidence | ||
| Rating | Definition | Rating | Definition |
| A | Strong | 1 | Based on published results of at least 1 randomized clinical trial with clinical outcomes or validated laboratory endpoints. |
| B | Moderate | * | Based on either a self-evident conclusion; conclusive, published, in vitro data; or well-established practice that cannot be tested because ethics would preclude a clinical trial. |
| C | Optional | 2 | Based on published results of at least 1 well-designed, nonrandomized clinical trial or observational cohort study with long-term clinical outcomes. |
| 2† | Extrapolated from published results of well-designed studies (including nonrandomized clinical trials) conducted in populations other than those specifically addressed by a recommendation. The source(s) of the extrapolated evidence and the rationale for the extrapolation are provided in the guideline text. One example would be results of studies conducted predominantly in a subpopulation (e.g., one gender) that the committee determines to be generalizable to the population under consideration in the guideline. | ||
| 3 | Based on committee expert opinion, with rationale provided in the guideline text. | ||
Last updated on June 10, 2026