
Purpose of This Guidance
Date of current publication: June 10, 2026
Lead author: Eugenia L. Siegler, MD
Writing group: Rona M. Vail, MD, AAHIVS; Sanjiv S. Shah, MD, MPH, AAHIVS; Steven M. Fine, MD, PhD; Joseph P. McGowan, MD, FACP, FIDSA, AAHIVS; Samuel T. Merrick, MD, FIDSA; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Anne K. Monroe, MD, MSPH; Jessica Rodrigues, MPH, MS; Christopher J. Hoffmann, MD, MPH, MSc, FACP; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: July 31, 2020
Purpose: Although published evidence-based strategies to support clinical recommendations are not currently available, a growing literature base describes evidence-informed and emerging strategies for the care of older populations with HIV or those who are long-term survivors of HIV. Based on the evidence, this guidance presents strategies to help clinicians recognize and address the needs of older patients with HIV Dunville and Greene 2025.
The goals of this guidance are to:
- Raise clinicians’ awareness of the needs and concerns of patients with HIV who are aged ≥50 years.
- Inform clinicians about an aging-related approach to older patients with HIV.
- Highlight good practices to help clinicians provide optimal care for this population.
- Provide resources about aging with HIV for clinicians and their patients.
- Offer models to guide medical settings in implementing geriatric care into HIV clinical practice.
Demographics: At the end of 2023, according to the Centers for Disease Control and Prevention, more than 53% of people with HIV in the United States were aged ≥50 years and more than 28% were aged ≥60 years CDC 2025. As of the end of 2024 in New York State, 56% of people with HIV were aged ≥50 years and one-third were aged ≥60 years NYSDOH 2025. That same year, almost 16% of new HIV diagnoses in New York State occurred in people aged ≥50 years, and nearly 29% of them had progressed to AIDS at the time of diagnosis NYSDOH 2025.
Ensuring appropriate care delivery: Although the effects of HIV on aging have been studied for years, HIV care has been acknowledged only recently as a domain of geriatrics Guaraldi and Rockwood 2017. Geriatric assessment provides a complete view of a patient’s function, cognition, and health, and improves prognostication and treatment decisions Singh, et al. 2017. As the population with HIV grows older, the application of the principles of geriatrics can enhance the quality of care.
Definition of terms:
- “Older”: Published studies differ in their definitions of older individuals with HIV (e.g., aged ≥50 years, ≥55 years, ≥60 years), and the needs of individuals within different age groups may differ markedly. This guidance defines older patients as those aged ≥50 years, which is the same definition used by the U.S. Department of Health and Human Services considerations for antiretroviral use in special populations DHHS 2024. Nonetheless, clinical programs may wish to distinguish different strata within this population, as their needs may differ; a local needs assessment is key to determining how best to care for this population as its age distribution continues to change.
- “Long-term survivor”: The term long-term survivor has different meanings. Some have defined it as having been diagnosed with HIV before the era of effective antiretroviral therapy amFAR 2022; others have defined it in terms of the length of time an individual has lived with HIV, e.g., for at least 1 or 2 decades. Long-term survivors can be any age. For example, older teens and adults who were perinatally infected are long-term survivors. It is useful to ask patients if they self-identify as long-term survivors and what that term means to them.
- “Lifetime survivor”: Adults who have acquired HIV perinatally are known as “lifetime survivors” (and as “Dandelions”). More than 30% of lifetime survivors are aged ≥30 years and, by definition, long-term survivors CDC 2024.
Effects of Aging
Long-term survivors appear to have physiologic changes consistent with advanced or accentuated aging Akusjarvi and Neogi 2023, even at the level of gene expression and modification Wallace, et al. 2026; Esteban-Cantos, et al. 2021; De Francesco, et al. 2019. When compared with age-matched controls who do not have HIV, older individuals with HIV have more comorbidities Verheij, et al. 2023 and polypharmacy Kong, et al. 2019; Guaraldi, et al. 2018; poorer bone health Lazcano, et al. 2025; Erlandson, et al. 2016; and higher rates of cognitive decline Goodkin, et al. 2017; Vance, et al. 2016, depression Do, et al. 2014, and aging-related syndromes, such as gait impairment and frailty Falutz 2020. Mental health can also be affected in many ways; in a study of individuals with HIV aged ≥50 years in San Francisco, the majority of participants reported loneliness, poor social support, and/or depression, and nearly half reported anxiety John, et al. 2016. Older individuals may also experience negative effects due to the stigma of ageism, which may be compounded by other kinds of stigma, such as racial, gender, or HIV-related stigma Guaraldi, et al. 2024; Johnson Shen, et al. 2019. In addition, long-term survivors, who may have expected to die at a young age like so many of their peers, may feel survivor’s guilt Machado 2012.
Long-term survivors are not necessarily chronologically old. Adult lifetime survivors, i.e., those who acquired HIV perinatally, are long-term survivors. Although they may be in their 20s, 30s, and 40s, they may show signs of advanced aging and age-related comorbidities Coker, et al. 2025; Mallik, et al. 2025, in addition to unique biological and psychosocial stressors. See NYSDOH AI guideline Primary Care for Adults With HIV > Goals of Primary Care for Adults With HIV > Lifetime Survivors.
These age-related concerns are not limited to long-term survivors. Although individuals who are aged ≥50 years with newly diagnosed HIV are not likely to exhibit the same degree of age advancement as those who have lived a long time with HIV, they may have a delayed diagnosis, low CD4 cell counts, and AIDS at the time of diagnosis Tavoschi, et al. 2017. Late initiation of antiretroviral therapy increases the long-term risk of complications Molina, et al. 2018.
Sex differences in the effect of HIV on aging remain an area of controversy. Studies in several countries have found that women with HIV have life expectancies closer to their HIV-negative counterparts than do men with HIV, but this finding has not been supported by studies in North America Pellegrino, et al. 2023; Wandeler, et al. 2016; Samji, et al. 2013. A Canadian study showed shorter life expectancy among women with HIV than men with HIV Hogg, et al. 2017. Women with HIV in resource-rich countries appear to have a heightened risk of comorbidities Palella, et al. 2019, including cardiovascular disease Kovacs, et al. 2022; Stone, et al. 2017, cognitive loss Maki, et al. 2018, and more rapid declines in bone mineral density Erlandson, et al. 2018. There may even be differences between men and women in HIV-related epigenetic changes Johnston, et al. 2025.
Approach to Aging in HIV Care
| GOOD PRACTICES |
Approach to Aging in HIV Care
|
Discuss aging-related concerns sensitively: It is essential to discuss aging-related concerns with patients with HIV who are aged ≥50 years or lifetime survivors. Some HIV clinicians and their patients have enduring relationships. Such longstanding ties promote high levels of trust, but they can also inhibit exploration of new concerns and promote too tight a focus on keeping viral load undetectable and treating common comorbidities. As a consequence, older individuals with HIV may not recognize concerns as aging-related or may feel it is unnecessary or inappropriate to discuss aging; they may find terms like “geriatric” or “geriatrician” upsetting or off-putting. Lifetime survivors, who may be in their 30s or 40s, likely have not thought about aging.
Care of older patients and lifetime survivors with HIV begins with recognizing that aging-related concerns are a fundamental part of primary care. Geriatric concerns do not supplant other medical conditions; they reframe them in light of a multiplicity of problems and a finite lifespan. A geriatric approach, even for people in their 50s or lifetime survivors, can improve the quality of care. People aging with HIV are a heterogeneous group. Providing care for these patients requires balance to avoid ageism and neglect of essential care while at the same time preventing excessive, dangerous, or unnecessary treatments. Determining what is appropriate for patients begins with an assessment of their health and their priorities.
Asking questions such as, “Have you thought about aging?” or “What would you like to know about aging with HIV?” creates opportunities to learn about patient’s concerns about the future and to discuss survivorship, guilt, ageism, financial worries, and other issues Del Carmen, et al. 2019. This is an opportunity to discuss healthy aging through lifestyle modifications that include exercise, diet, and socialization.
Sexual health: Older age does not preclude discussions of topics that are essential to health. For example, sexuality should be considered an essential part of health at any age. There is no age limit at which clinicians should stop taking a sexual history or discussing HIV pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP) for partners. Initiating discussions of sexual health, including topics such as erectile dysfunction and loss of libido in men, menopause and postmenopausal sex in women, the importance of safer sex practices, and screening for sexually transmitted infections as needed, may also provide insights into relationships and the strength of a patient’s social network. For more information, see the GOALS Approach to Sexual History and Health.
Cancer screening: Overall, patient health and priorities, rather than age, direct the frequency of cancer screening in individuals with HIV. The literature on adherence to cancer screening guidelines among individuals with HIV is mixed, with most Corrigan, et al. 2019 but not all Barnes, et al. 2018 studies failing to find that older individuals were screened less frequently. In patients with a good prognosis, clinicians should continue to follow screening guidelines (see the NYSDOH AI guideline Primary Care for Adults With HIV > HIV-Specific Primary Care). Screening can be re-evaluated when it conflicts with a patient’s priorities or when a patient’s prognosis is poor.
Aging-related syndromes: Some health concerns take on greater relevance as individuals with HIV age. Geriatric or aging-related syndromes, such as frailty, have received special attention. Frailty, which can be measured as a physical construct or as an “accumulation of deficits,” is a measure of vulnerability Zhabokritsky and Falutz 2025; Kehler, et al. 2022. Frailty has been associated with increases in falls Erlandson, et al. 2019 and mortality Piggott, et al. 2020; Kelly, et al. 2019, and multiple comorbidities Masters, et al. 2021; Kelly, et al. 2019 have been linked to its development. However, it is possible to reverse frailty Zhabokritsky and Falutz 2025. Early identification may enable increased resources for those at highest risk and may also draw attention to associated comorbidities.
Comorbidities: Management of comorbidities should follow the recommendations and guidance found in the NYSDOH AI guideline Primary Care for Adults With HIV > HIV-Specific Primary Care. For older patients, cognitive impairment and impaired bone health merit special mention:
- Cognitive impairment: People with HIV are at higher risk of cognitive impairment than those without HIV Bobrow, et al. 2020. HIV “legacy effects” remain important, but an international workshop has suggested that the term HABI (HIV-associated brain injury) replace HAND (HIV-associated neurocognitive disease) given the multifactorial nature of cognitive impairment Winston, et al. 2025; Nightingale, et al. 2023. Although effective antiretroviral therapy (ART) has significantly reduced the prevalence of HIV-associated dementias, comorbidities and neurodegenerative diseases have a large effect on cognition as the population with HIV ages. In addition to the early initiation of effective ART, many opportunities to prevent or mitigate cognitive decline are available, including aggressive management of cardiovascular disease and hypertension and elimination or reduction of polypharmacy Korpela, et al. 2026 and anticholinergic and other neurotoxic medications. Stabilization of cognitive impairment in people with HIV may be possible through multidisciplinary interventions Alford, et al. 2026. A recent review for the general population suggests multiple opportunities for prevention throughout the lifespan Livingston, et al. 2024.
- Poor bone health: People with HIV are at higher risk of osteoporosis and fractures compared with age-matched controls Starup-Linde, et al. 2020. Guidelines for bone mineral density testing are available (see Table 1: Assessment Domains for Older People With HIV and Selected Tools and Resources) but are often not followed Birabaharan, et al. 2021; Starup-Linde, et al. 2020. Treatments and preventive care should include modalities such as diet and exercise in addition to pharmacologic therapy Hasenmajer, et al. 2025.
Nonpharmacologic approaches to health: Nonpharmacologic components are essential to care plans. A variety of modalities are evidence-based de Luque, et al. 2025, and others are under study in people with HIV. Exercise appears to improve or stabilize a number of health outcomes, including physical function Kulik, et al. 2026; Su, et al. 2026, sarcopenia SeyedAlinaghi, et al. 2025, bone health Grutter Lopes, et al. 2024, vascular health Jones, et al. 2024, mood Heissel, et al. 2019, and cognition Cooley, et al. 2026; Quigley, et al. 2019. “Food as Medicine” can also improve health outcomes Berkowitz, et al. 2025; Palar, et al. 2025.
Insurance and long-term care needs: Addressing aging-related concerns directly can help older patients with HIV discuss financial worries and prepare for the future when more personal assistance may be needed. Discussing insurance coverage with patients with HIV when they are in their 60s provides an opportunity to help them prepare for the transition from commercial insurance, Medicaid, or SNPs to Medicare-based plans. Planning is essential because commercial insurance plans or SNPs often offer more comprehensive care coordination, medication coverage, and health-maintenance services than Medicare-based plans. People with HIV may need long-term care at an earlier age than those without HIV Justice and Akgun 2019. Open discussion about support systems can help patients begin to plan for their long-term care needs.
The 5Ms—an effective communication tool: The geriatric approach can be described as attention to the 5Ms: mind, mobility, multimorbidity, medications, and matters most Tinetti, et al. 2017. The 5Ms are a useful way to communicate geriatric principles or choose an area for screening. However, some aging-related syndromes (e.g., dizziness, incontinence) or activities of daily living may not easily fit into one of these categories. Nor do the 5Ms offer a structure for a comprehensive geriatric assessment. The following discussion addresses how the 5Ms can be used to understand and explain geriatric priorities and broaden the focus beyond specific comorbidities. The 5Ms are best viewed as an explanatory framework; it is important that screening and assessment be performed with formally recognized instruments (see Table 1: Assessment Domains for Older People With HIV and Selected Tools and Resources).
1. Mind: This category includes all domains of behavioral health, including cognition, mood, and other disorders. General assessment questions about instrumental activities of daily living (e.g., using transportation, managing medications, and handling finances) can provide information about practical concerns and offer clues about cognitive or emotional barriers to self-care. Clinicians can also use specific tools (see Table 1) to screen patients for disorders such as depression or cognitive impairment, which may be caused by factors both related to and independent of HIV Winston and Spudich 2020. Even as the prevalence of HIV-associated neurocognitive disorder has decreased among individuals with HIV, having multiple comorbidities can increase the risk of cognitive impairment Heaton, et al. 2023. Identifying factors that can be addressed to prevent or slow cognitive deterioration is a fundamental part of assessment in this category.
2. Mobility: Clinicians can begin to address mobility with a general assessment of activities of daily living to determine whether patients have difficulty dressing or bathing. Discussion of a patient’s fall risk can begin with a question such as, “Have you fallen in the past year?” or clinicians can use a comprehensive fall-risk screening tool. The value of exercise, both structured and informal de Luque, et al. 2025, is a key area for discussion.
3. Multimorbidity: Care for older patients with HIV usually involves the management of multiple comorbidities, each of which may require treatment with multiple medications. Nonpharmacologic management (e.g., smoking cessation, dietary modification, exercise) can also improve symptoms associated with multiple comorbidities Fitch 2019.
A geriatric perspective recognizes that, in patients with multimorbidity, strict adherence to multiple disease-based treatment guidelines may not be possible or may jeopardize a patient’s health. Simultaneous management of multiple chronic conditions necessitates establishing treatment priorities Yarnall, et al. 2017, which requires understanding a patient’s priorities Tinetti, et al. 2019.
4. Medications:While older individuals with HIV are taking antiretroviral medications to suppress the virus, they may also be taking other medications to treat comorbidities, which can make medication management especially challenging. Polypharmacy is common, and women appear to be at higher risk than men, likely because of a higher prevalence of comorbidities Livio, et al. 2021. Polypharmacy may be unavoidable and even appropriate in the context of multiple comorbidities; strategies that can help reduce medication risk include focusing on potentially inappropriate medications Sukumaran, et al. 2026 and avoiding anticholinergic medications. Medication evaluation should include a review of all medications, potential drug-drug interactions Livio and Marzolini 2019, and short- and long-term toxic effects. It may be beneficial to simplify antiretroviral and other medication regimens to ensure that harms from drug-drug interactions and other adverse effects of treatment are avoided Del Carmen, et al. 2019; older people with HIV may be open to discussion of newer long-acting and/or injectable ART regimens, if indicated Mendes de Leon, et al. 2025. Caution is required when adjusting or simplifying ART regimens if changes involve either initiating or discontinuing a medication with pharmacologic inhibitive or induction actions; these changes may affect levels of coadministered medications.
Consultation with a pharmacist Ahmed, et al. 2023 or polypharmacy clinic Cattaneo, et al. 2023; Halli-Tierney, et al. 2019 can reduce drug-drug interactions and polypharmacy and help clinicians navigate the complexities of medication management in older patients. The University of Liverpool HIV Drug Interactions Checker is a useful tool for checking drug-drug interactions; also see NYSDOH AI resource Drug-Drug Interaction Guide: From HIV Prevention to Treatment.
5. Matters most: This is the broadest category and includes medical and social priorities, sexual health, and advance directives. This category also includes discussion of palliative care Tamsukhin, et al. 2024 and frank discussion of long-term care needs and end-of-life plans. Advance directives should be addressed and, if an advance directive is in place, revisited. It is preferable for the patient to designate a specific agent or agents who can speak for them when they are incapacitated. Patients who cannot or will not identify a trusted individual to be their agent can complete the NYSDOH Medical Orders for Life-Sustaining Treatment (MOLST) to describe their wishes regarding medical treatment. The MOLST can now also be documented electronically in the eMOLST registry.
Geriatric Screening and Assessment
General Screening Tools
Screening identifies individuals who are at risk of medical problems. Although clinicians may order screening tests for specific diseases such as cancer, they may not be as familiar with screening tools designed to identify functional impairment or geriatric syndromes. In all cases, the same principles apply: brief, sensitive geriatric screening instruments such as those included in Box 1, below, can be used to identify patients who may need more intensive evaluation.
For those programs that are just starting to identify the needs of their older patients, a general screening questionnaire is an excellent place to start. General screening questionnaires are usually appropriate for all older patients and long-term survivors and often are performed annually around a patient’s birthday. Such screenings can be completed before a clinic visit; some questionnaires are completed by the patient and others are administered by a staff member. The modified World Health Organization integrated care for older people (ICOPE) screening tool has been tested for people with HIV in a New York State-wide pilot and can be administered by staff in person or over the phone; sites can also use other surveys based on workflows.
Why perform general geriatric screening? Not every patient requires a formal geriatric assessment. Tools for general geriatric screening are simple and cover a wide variety of domains; if the results indicate that more extensive assessment is warranted, then a more formal and comprehensive evaluation can be performed. Use of general screening tools can improve case-finding and, when coupled with referral, can enable targeted interventions but has not yet been shown to reduce hospitalizations or improve function Rubenstein, et al. 2007.
| Box 1: General Geriatric Screening Tools for Older Adults With HIV |
|
Comprehensive Geriatric Assessment
When a patient has a positive result on a general geriatric screening test, the clinician may consider a more comprehensive assessment using validated tools. Formal assessment is more effective than clinical judgment at uncovering problems Elam, et al. 1991; Pinholt, et al. 1987.
The Comprehensive Geriatric Assessment: The gold standard for geriatric evaluation is the Comprehensive Geriatric Assessment (CGA), which assesses multiple domains of health and function Singh, et al. 2017. Because it is comprehensive, the CGA is lengthy, and its use may not be feasible in many clinical settings. In the general geriatric outpatient setting, the CGA has not been shown to reduce mortality or nursing home placement, although it may reduce hospital admissions Briggs, et al. 2022. The CGA is a complicated process, requiring both expert assessors and clear care plans to manage areas of deficit, and its mixed success in the community likely stems at least in part from the complexity of creating a system that effectively responds to the assessment and includes patient buy-in.
Consulting experts in geriatric care: Some academic centers have tested models of collaboration with geriatricians Davis, et al. 2022, including referral to geriatric consultants outside the practice, multidisciplinary geriatric care within the practice, and dual training of clinicians in geriatrics and HIV medicine. Geriatric Workforce Enhancement Programs, funded by the Health Resources and Services Administration, can offer training and access to geriatric expertise.
Choosing domains for focused assessment: Given the limitations in both the HIV care and geriatrics workforces Armstrong 2021; American Geriatrics Society 2017, access to geriatricians may not be feasible. Community-based programs wishing to assess specific domains in the absence of available expert clinicians may choose from among many options.
Recommendations from community advisory boards and patient surveys can advise sites about patient priorities, and results from general screenings can prompt more broad assessments to identify high-prevalence problems. It may be difficult to implement needed aging-related assessments when access to expertise or funding is limited, but every attempt should be made to assess aging-related concerns to the degree possible. Table 1, below, lists domains of geriatric assessment and selected resources for older patients with HIV.
Integrating the Needs of Older Patients Into Medical Care
This guidance is designed to broaden the clinician’s perspective, improving care for older patients with HIV. However, the HIV clinician cannot provide optimal care in the absence of practice change. Clinical practices can begin to address HIV-related aging concerns by taking the steps outlined in Box 2, below.
Models of care for people aging with HIV: Although initial efforts focused on developing or linking to physician geriatric expertise Davis, et al. 2022, more recent programs have expanded the breadth of services and focused on clinic-wide change. These models, including those developed through the Human Resources and Services Administration-funded Special Projects of National Significance Aging with HIV Initiative and the NYSDOH AI People Aging with HIV (PAWH) Pilot Program, along with others from England St Clair-Sullivan, et al. 2026; Varadarajan, et al. 2025, described evidence-informed, more comprehensive options Dunville and Greene 2025. Two keys to sustainability of any program, irrespective of size, are buy-in from staff and linkage to programs and services that will help remediate the problems uncovered by screening and/or geriatric assessment.
| Box 2: Six Steps to Integrating Needs of Older Patients Into HIV Medical Care |
| 1. Assess the clinic’s ability to meet the needs of older patients with HIV through practice change: |
|
| 2. Engage older patients with HIV in program planning: |
|
| 3. Consider options and develop protocols for identifying patients in need of aging-related care and services. For example, patients may be identified based on: |
|
| 4. Develop an assessment strategy: |
|
| 5. Develop protocols for referral: |
|
| 6. Link to the Aging Network for services: |
|
| ONLINE RESOURCES FOR AGING AND GERIATRIC CARE |
Clinical Resources:
Services and Entitlements:
|
Shared Decision-Making
Download Printable PDF of Shared Decision-Making Statement
Date of current publication: August 8, 2023
Lead authors: Jessica Rodrigues, MS; Jessica M. Atrio, MD, MSc; and Johanna L. Gribble, MA
Writing group: Steven M. Fine, MD, PhD; Rona M. Vail, MD; Samuel T. Merrick, MD; Asa E. Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee: Medical Care Criteria Committee
Date of original publication: August 8, 2023
Rationale
Throughout its guidelines, the New York State Department of Health (NYSDOH) AIDS Institute (AI) Clinical Guidelines Program recommends “shared decision-making,” an individualized process central to patient-centered care. With shared decision-making, clinicians and patients engage in meaningful dialogue to arrive at an informed, collaborative decision about a patient’s health, care, and treatment planning. The approach to shared decision-making described here applies to recommendations included in all program guidelines. The included elements are drawn from a comprehensive review of multiple sources and similar attempts to define shared decision-making, including the Institute of Medicine’s original description [Institute of Medicine 2001]. For more information, a variety of informative resources and suggested readings are included at the end of the discussion.
Benefits
The benefits to patients that have been associated with a shared decision-making approach include:
- Decreased anxiety [Niburski, et al. 2020; Stalnikowicz and Brezis 2020]
- Increased trust in clinicians [Acree, et al. 2020; Groot, et al. 2020; Stalnikowicz and Brezis 2020]
- Improved engagement in preventive care [McNulty, et al. 2022; Scalia, et al. 2022; Bertakis and Azari 2011]
- Improved treatment adherence, clinical outcomes, and satisfaction with care [Crawford, et al. 2021; Bertakis and Azari 2011; Robinson, et al. 2008]
- Increased knowledge, confidence, empowerment, and self-efficacy [Chen, et al. 2021; Coronado-Vázquez, et al. 2020; Niburski, et al. 2020]
Approach
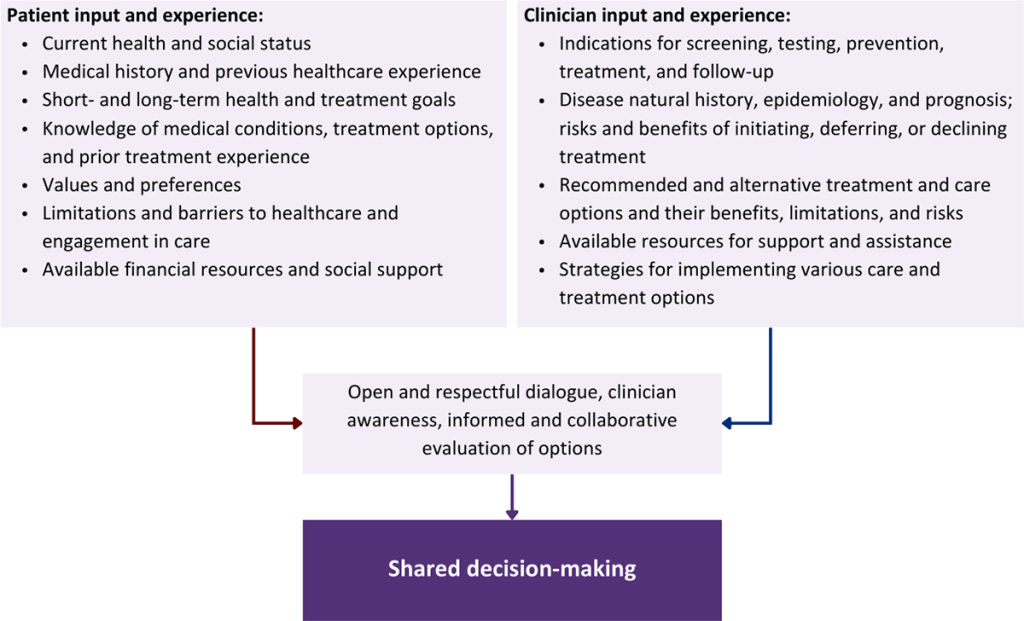
Collaborative care: Shared decision-making is an approach to healthcare delivery that respects a patient’s autonomy in responding to a clinician’s recommendations and facilitates dynamic, personalized, and collaborative care. Through this process, a clinician engages a patient in an open and respectful dialogue to elicit the patient’s knowledge, experience, healthcare goals, daily routine, lifestyle, support system, cultural and personal identity, and attitudes toward behavior, treatment, and risk. With this information and the clinician’s clinical expertise, the patient and clinician can collaborate to identify, evaluate, and choose from among available healthcare options [Coulter and Collins 2011]. This process emphasizes the importance of a patient’s values, preferences, needs, social context, and lived experience in evaluating the known benefits, risks, and limitations of a clinician’s recommendations for screening, prevention, treatment, and follow-up. As a result, shared decision-making also respects a patient’s autonomy, agency, and capacity in defining and managing their healthcare goals. Building a clinician-patient relationship rooted in shared decision-making can help clinicians engage in productive discussions with patients whose decisions may not align with optimal health outcomes. Fostering open and honest dialogue to understand a patient’s motivations while suspending judgment to reduce harm and explore alternatives is particularly vital when a patient chooses to engage in practices that may exacerbate or complicate health conditions [Halperin, et al. 2007].
Options: Implicit in the shared decision-making process is the recognition that the “right” healthcare decisions are those made by informed patients and clinicians working toward patient-centered and defined healthcare goals. When multiple options are available, shared decision-making encourages thoughtful discussion of the potential benefits and potential harms of all options, which may include doing nothing or waiting. This approach also acknowledges that efficacy may not be the most important factor in a patient’s preferences and choices [Sewell, et al. 2021].
Clinician awareness: The collaborative process of shared decision-making is enhanced by a clinician’s ability to demonstrate empathic interest in the patient, avoid stigmatizing language, employ cultural humility, recognize systemic barriers to equitable outcomes, and practice strategies of self-awareness and mitigation against implicit personal biases [Parish, et al. 2019].
Caveats: It is important for clinicians to recognize and be sensitive to the inherent power and influence they maintain throughout their interactions with patients. A clinician’s identity and community affiliations may influence their ability to navigate the shared decision-making process and develop a therapeutic alliance with the patient and may affect the treatment plan [KFF 2023; Greenwood, et al. 2020]. Furthermore, institutional policy and regional legislation, such as requirements for parental consent for gender-affirming care for transgender people or insurance coverage for sexual health care, may infringe upon a patient’s ability to access preventive- or treatment-related care [Sewell, et al. 2021].
Figure 1: Elements of Shared Decision-Making
Health equity: Adapting a shared decision-making approach that supports diverse populations is necessary to achieve more equitable and inclusive health outcomes [Castaneda-Guarderas, et al. 2016]. For instance, clinicians may need to incorporate cultural- and community-specific considerations into discussions with women, gender-diverse individuals, and young people concerning their sexual behaviors, fertility intentions, and pregnancy or lactation status. Shared decision-making offers an opportunity to build trust among marginalized and disenfranchised communities by validating their symptoms, values, and lived experience. Furthermore, it can allow for improved consistency in patient screening and assessment of prevention options and treatment plans, which can reduce the influence of social constructs and implicit bias [Castaneda-Guarderas, et al. 2016].
Clinician bias has been associated with health disparities and can have profoundly negative effects [FitzGerald and Hurst 2017; Hall, et al. 2015]. It is often challenging for clinicians to recognize and set aside personal biases and to address biases with peers and colleagues. Consciously or unconsciously, negative or stigmatizing assumptions are often made about patient characteristics, such as race, ethnicity, gender, sexual orientation, mental health, and substance use [Avery, et al. 2019; van Boekel, et al. 2013; Livingston, et al. 2012]. With its emphasis on eliciting patient information, a shared decision-making approach encourages clinicians to inquire about patients’ lived experiences rather than making assumptions and to recognize the influence of that experience in healthcare decision-making.
Stigma: Stigma may prevent individuals from seeking or receiving treatment and harm reduction services [Tsai, et al. 2019]. Among people with HIV, stigma and medical mistrust remain significant barriers to healthcare utilization, HIV diagnosis, and medication adherence and can affect disease outcomes [Turan, et al. 2017; Chambers, et al. 2015], and stigma among clinicians against people who use substances has been well-documented [Stone, et al. 2021; Tsai, et al. 2019; van Boekel, et al. 2013]. Sexual and reproductive health, including strategies to prevent HIV transmission, acquisition, and progression, may be subject to stigma, bias, social influence, and violence.
| SHARED DECISION-MAKING IN HIV CARE |
|
Resources and Suggested Reading
In addition to the references cited below, the following resources and suggested reading may be useful to clinicians.
| RESOURCES |
References
Acree ME, McNulty M, Blocker O, et al. Shared decision-making around anal cancer screening among black bisexual and gay men in the USA. Cult Health Sex 2020;22(2):201-16. [PMID: 30931831]
Avery JD, Taylor KE, Kast KA, et al. Attitudes toward individuals with mental illness and substance use disorders among resident physicians. Prim Care Companion CNS Disord 2019;21(1):18m02382. [PMID: 30620451]
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med 2011;24(3):229-39. [PMID: 21551394]
Castaneda-Guarderas A, Glassberg J, Grudzen CR, et al. Shared decision making with vulnerable populations in the emergency department. Acad Emerg Med 2016;23(12):1410-16. [PMID: 27860022]
Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health 2015;15:848. [PMID: 26334626]
Chen CH, Kang YN, Chiu PY, et al. Effectiveness of shared decision-making intervention in patients with lumbar degenerative diseases: a randomized controlled trial. Patient Educ Couns 2021;104(10):2498-2504. [PMID: 33741234]
Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, et al. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore) 2020;99(32):e21389. [PMID: 32769870]
Coulter A, Collins A. Making shared decision-making a reality: no decision about me, without me. 2011. https://www.kingsfund.org.uk/sites/default/files/Making-shared-decision-making-a-reality-paper-Angela-Coulter-Alf-Collins-July-2011_0.pdf
Crawford J, Petrie K, Harvey SB. Shared decision-making and the implementation of treatment recommendations for depression. Patient Educ Couns 2021;104(8):2119-21. [PMID: 33563500]
FitzGerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics 2017;18(1):19. [PMID: 28249596]
Greenwood BN, Hardeman RR, Huang L, et al. Physician-patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci U S A 2020;117(35):21194-21200. [PMID: 32817561]
Groot G, Waldron T, Barreno L, et al. Trust and world view in shared decision making with indigenous patients: a realist synthesis. J Eval Clin Pract 2020;26(2):503-14. [PMID: 31750600]
Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health 2015;105(12):e60-76. [PMID: 26469668]
Halperin B, Melnychuk R, Downie J, et al. When is it permissible to dismiss a family who refuses vaccines? Legal, ethical and public health perspectives. Paediatr Child Health 2007;12(10):843-45. [PMID: 19043497]
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. 2001. https://www.ncbi.nlm.nih.gov/books/NBK222274/
KFF. Key data on health and health care by race and ethnicity. 2023 Mar 15. https://www.kff.org/racial-equity-and-health-policy/report/key-data-on-health-and-health-care-by-race-and-ethnicity/ [accessed 2023 May 19]
Livingston JD, Milne T, Fang ML, et al. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction 2012;107(1):39-50. [PMID: 21815959]
McNulty MC, Acree ME, Kerman J, et al. Shared decision making for HIV pre-exposure prophylaxis (PrEP) with black transgender women. Cult Health Sex 2022;24(8):1033-46. [PMID: 33983866]
Niburski K, Guadagno E, Abbasgholizadeh-Rahimi S, et al. Shared decision making in surgery: a meta-analysis of existing literature. Patient 2020;13(6):667-81. [PMID: 32880820]
Parish SJ, Hahn SR, Goldstein SW, et al. The International Society for the Study of Women’s Sexual Health process of care for the identification of sexual concerns and problems in women. Mayo Clin Proc 2019;94(5):842-56. [PMID: 30954288]
Robinson JH, Callister LC, Berry JA, et al. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008;20(12):600-607. [PMID: 19120591]
Scalia P, Durand MA, Elwyn G. Shared decision-making interventions: an overview and a meta-analysis of their impact on vaccine uptake. J Intern Med 2022;291(4):408-25. [PMID: 34700363]
Sewell WC, Solleveld P, Seidman D, et al. Patient-led decision-making for HIV preexposure prophylaxis. Curr HIV/AIDS Rep 2021;18(1):48-56. [PMID: 33417201]
Stalnikowicz R, Brezis M. Meaningful shared decision-making: complex process demanding cognitive and emotional skills. J Eval Clin Pract 2020;26(2):431-38. [PMID: 31989727]
Stone EM, Kennedy-Hendricks A, Barry CL, et al. The role of stigma in U.S. primary care physicians’ treatment of opioid use disorder. Drug Alcohol Depend 2021;221:108627. [PMID: 33621805]
Tsai AC, Kiang MV, Barnett ML, et al. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med 2019;16(11):e1002969. [PMID: 31770387]
Turan B, Budhwani H, Fazeli PL, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav 2017;21(1):283-91. [PMID: 27272742]
van Boekel LC, Brouwers EP, van Weeghel J, et al. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug Alcohol Depend 2013;131(1-2):23-35. [PMID: 23490450]
References
Ahmed A., Tanveer M., Dujaili J. A., et al. Pharmacist-involved antiretroviral stewardship programs in people living with HIV/AIDS: a systematic review. AIDS Patient Care STDS 2023;37(1):31-52. [PMID: 36626156]
Akusjarvi S. S., Neogi U. Biological aging in people living with HIV on successful antiretroviral therapy: do they age faster?. Curr HIV/AIDS Rep 2023;20(2):42-50. [PMID: 36695947]
Alford K., Fitzpatrick C., Rhodes S., et al. Addressing cognitive symptoms in people with HIV: outcomes from a holistic screening and management pathway. J Acquir Immune Defic Syndr 2026;101(2):199-207. [PMID: 41060051]
American Geriatrics Society. Projected future need for geriatricians. 2017 Mar. https://www.americangeriatrics.org/sites/default/files/inline-files/Projected-Future-Need-for-Geriatricians_1.pdf [accessed 2026 Mar 5]
American Geriatrics Society. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2023;71(7):2052-81. [PMID: 37139824]
amFAR. In the spotlight: long-term survivors. 2022 Jun 4. https://www.amfar.org/news/long-term-survivors/ [accessed 2025 Mar 5]
Armstrong W. S. The human immunodeficiency virus workforce in crisis: an urgent need to build the foundation required to end the epidemic. Clin Infect Dis 2021;72(9):1627-30. [PMID: 32211784]
Barnes A., Betts A. C., Borton E. K., et al. Cervical cancer screening among HIV-infected women in an urban, United States safety-net healthcare system. AIDS 2018;32(13):1861-70. [PMID: 29762164]
Berkowitz S. A., Seligman H. K., Mozaffarian D. A new approach to guide research and policy at the intersection of income, food, nutrition, and health. Health Aff (Millwood) 2025;44(4):384-90. [PMID: 40193831]
Birabaharan M., Kaelber D. C., Karris M. Y. Bone mineral density screening among people with HIV: a population-based analysis in the United States. Open Forum Infect Dis 2021;8(3):ofab081. [PMID: 33796595]
Biver E., Calmy A., Aubry-Rozier B., et al. Diagnosis, prevention, and treatment of bone fragility in people living with HIV: a position statement from the Swiss Association Against Osteoporosis. Osteoporos Int 2019;30(5):1125-35. [PMID: 30603840]
Bobrow K., Xia F., Hoang T., et al. HIV and risk of dementia in older veterans. AIDS 2020;34(11):1673-79. [PMID: 32701576]
Boyd C., Smith C. D., Masoudi F. A., et al. Decision making for older adults with multiple chronic conditions: executive summary for the American Geriatrics Society Guiding Principles on the Care of Older Adults With Multimorbidity. J Am Geriatr Soc 2019;67(4):665-73. [PMID: 30663782]
Briggs R., McDonough A., Ellis G., et al. Comprehensive Geriatric Assessment for community-dwelling, high-risk, frail, older people. Cochrane Database Syst Rev 2022;5(5):CD012705. [PMID: 35521829]
Bruce R. D., Merlin J., Lum P. J., et al. 2017 HIVMA of IDSA clinical practice guideline for the management of chronic pain in patients living with HIV. Clin Infect Dis 2017;65(10):e1-37. [PMID: 29020263]
Cattaneo D., Oreni L., Meraviglia P., et al. Polypharmacy and aging in people living with HIV: 6 years of experience in a multidisciplinary outpatient clinic. Drugs Aging 2023;40(7):665-74. [PMID: 37310576]
CDC. Diagnoses, deaths, and prevalence of HIV in the United States and 6 territories and freely associated states, 2022. 2024 May 21. https://stacks.cdc.gov/view/cdc/156509 [accessed 2026 Mar 5]
CDC. HIV data: HIV diagnoses, deaths, and prevalence. 2025 Feb 7. https://www.cdc.gov/hiv-data/nhss/hiv-diagnoses-deaths-prevalence.html [accessed 2026 Mar 5]
Coker M. O., Kreutzberg R., Sam-Agudu N. A., et al. The state of the science on chronic comorbidities and aging in children and adolescents with perinatally-acquired HIV. Curr HIV/AIDS Rep 2025;22(1):56. [PMID: 41351790]
Cooley S. A., Ferreiro A., Nelson B., et al. A randomized controlled trial to unveil the influence of an exercise intervention on brain integrity and gut microbiome structure in individuals with HIV. AIDS 2026;40(1):24-34. [PMID: 40965137]
Corrigan K. L., Wall K. C., Bartlett J. A., et al. Cancer disparities in people with HIV: a systematic review of screening for non-AIDS-defining malignancies. Cancer 2019;125(6):843-53. [PMID: 30645766]
Davis A. J., Greene M., Siegler E., et al. Strengths and challenges of various models of geriatric consultation for older adults living with human immunodeficiency virus. Clin Infect Dis 2022;74(6):1101-6. [PMID: 34358303]
De Francesco D., Wit F. W., Bürkle A., et al. Do people living with HIV experience greater age advancement than their HIV-negative counterparts?. AIDS 2019;33(2):259-68. [PMID: 30325781]
de Luque C. M. C., Sánchez-Conde M., Brañas F. Nonpharmacologic interventions to improve quality of life of older adults with HIV. Curr Opin HIV AIDS 2025;20(4):402-8. [PMID: 40171894]
Del Carmen T., Johnston C., Burchett C., et al. Special topics in the care of older people with HIV. Curr Treat Options Infect Dis 2019;11(4):388-400. [PMID: 33343235]
DHHS. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV: considerations for antiretroviral use in special populations: HIV and the older person. 2024 Sep 12. https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/special-populations-hiv-and-older-person [accessed 2026 Mar 5]
Do A. N., Rosenberg E. S., Sullivan P. S., et al. Excess burden of depression among HIV-infected persons receiving medical care in the United States: data from the Medical Monitoring Project and the Behavioral Risk Factor Surveillance System. PLoS One 2014;9(3):e92842. [PMID: 24663122]
Dunville R., Greene M. Innovative models of care supporting people aging with HIV. Curr Opin HIV AIDS 2025;20(4):367-72. [PMID: 40171890]
Elam J. T., Graney M. J., Beaver T., et al. Comparison of subjective ratings of function with observed functional ability of frail older persons. Am J Public Health 1991;81(9):1127-30. [PMID: 1951822]
Erlandson K. M., Guaraldi G., Falutz J. More than osteoporosis: age-specific issues in bone health. Curr Opin HIV AIDS 2016;11(3):343-50. [PMID: 26882460]
Erlandson K. M., Lake J. E., Sim M., et al. Bone mineral density declines twice as quickly among HIV-infected women compared with men. J Acquir Immune Defic Syndr 2018;77(3):288-94. [PMID: 29140875]
Erlandson K. M., Perez J., Abdo M., et al. Frailty, neurocognitive impairment, or both in predicting poor health outcomes among adults living with human immunodeficiency virus. Clin Infect Dis 2019;68(1):131-38. [PMID: 29788039]
Esteban-Cantos A., Rodriguez-Centeno J., Barruz P., et al. Epigenetic age acceleration changes 2 years after antiretroviral therapy initiation in adults with HIV: a substudy of the NEAT001/ANRS143 randomised trial. Lancet HIV 2021;8(4):e197-205. [PMID: 33794182]
Falutz J. Frailty in people living with HIV. Curr HIV/AIDS Rep 2020;17(3):226-36. [PMID: 32394155]
Fitch K. V. Contemporary lifestyle modification interventions to improve metabolic comorbidities in HIV. Curr HIV/AIDS Rep 2019;16(6):482-91. [PMID: 31776973]
Goodkin K., Miller E. N., Cox C., et al. Effect of ageing on neurocognitive function by stage of HIV infection: evidence from the Multicenter AIDS Cohort Study. Lancet HIV 2017;4(9):e411-22. [PMID: 28716545]
Greene M., Covinsky K. E., Valcour V., et al. Geriatric syndromes in older HIV-infected adults. J Acquir Immune Defic Syndr 2015;69(2):161-67. [PMID: 26009828]
Grutter Lopes K., Andrade Paz G., Farinatti P., et al. Effects of exercise training on bone health in adults living with HIV: a systematic review with meta-analysis. AIDS Care 2024;36(10):1400-1409. [PMID: 38502603]
Guaraldi G., Malagoli A., Calcagno A., et al. The increasing burden and complexity of multi-morbidity and polypharmacy in geriatric HIV patients: a cross sectional study of people aged 65 - 74 years and more than 75 years. BMC Geriatr 2018;18(1):99. [PMID: 29678160]
Guaraldi G., Milic J., Cascio M., et al. Ageism: the -ism affecting the lives of older people living with HIV. Lancet HIV 2024;11(1):e52-59. [PMID: 38040011]
Guaraldi G., Rockwood K. Geriatric-HIV medicine is born. Clin Infect Dis 2017;65(3):507-9. [PMID: 28387817]
Halli-Tierney A. D., Scarbrough C., Carroll D. Polypharmacy: evaluating risks and deprescribing. Am Fam Physician 2019;100(1):32-38. [PMID: 31259501]
Hasenmajer V., D'Addario N. F., Bonaventura I., et al. Breaking down bone disease in people living with HIV: pathophysiology, diagnosis, and treatment. Adv Exp Med Biol 2025;1476:87-110. [PMID: 39668274]
Heaton R. K., Ellis R. J., Tang B., et al. Twelve-year neurocognitive decline in HIV is associated with comorbidities, not age: a CHARTER study. Brain 2023;146(3):1121-31. [PMID: 36477867]
Heissel A., Zech P., Rapp M. A., et al. Effects of exercise on depression and anxiety in persons living with HIV: a meta-analysis. J Psychosom Res 2019;126:109823. [PMID: 31518734]
Hogg R. S., Eyawo O., Collins A. B., et al. Health-adjusted life expectancy in HIV-positive and HIV-negative men and women in British Columbia, Canada: a population-based observational cohort study. Lancet HIV 2017;4(6):e270-76. [PMID: 28262574]
Hu J. S., Pierre E. F. Urinary incontinence in women: evaluation and management. Am Fam Physician 2019;100(6):339-48. [PMID: 31524367]
John M. D., Greene M., Hessol N. A., et al. Geriatric assessments and association with VACS Index among HIV-infected older adults in San Francisco. J Acquir Immune Defic Syndr 2016;72(5):534-41. [PMID: 27028497]
Johnson Shen M., Freeman R., Karpiak S., et al. The intersectionality of stigmas among key populations of older adults affected by HIV: a thematic analysis. Clin Gerontol 2019;42(2):137-49. [PMID: 29617194]
Johnston C. D., Pang A. P. S., Siegler E. L., et al. Sex differences in epigenetic ageing for older people living with HIV. EBioMedicine 2025;113:105588. [PMID: 39923742]
Jones R., Robinson A. T., Beach L. B., et al. Exercise to prevent accelerated vascular aging in people living with HIV. Circ Res 2024;134(11):1607-35. [PMID: 38781293]
Justice A. C., Akgun K. M. What does aging with HIV mean for nursing homes?. J Am Geriatr Soc 2019;67(7):1327-29. [PMID: 31063666]
Kehler D. S., Milic J., Guaraldi G., et al. Frailty in older people living with HIV: current status and clinical management. BMC Geriatr 2022;22(1):919. [PMID: 36447144]
Kelly S. G., Wu K., Tassiopoulos K., et al. Frailty is an independent risk factor for mortality, cardiovascular disease, bone disease, and diabetes among aging adults with human immunodeficiency virus. Clin Infect Dis 2019;69(8):1370-76. [PMID: 30590451]
Koethe J. R., Lagathu C., Lake J. E., et al. HIV and antiretroviral therapy-related fat alterations. Nat Rev Dis Primers 2020;6(1):48. [PMID: 32555389]
Kong A. M., Pozen A., Anastos K., et al. Non-HIV comorbid conditions and polypharmacy among people living with HIV age 65 or older compared with HIV-negative individuals age 65 or older in the United States: a retrospective claims-based analysis. AIDS Patient Care STDS 2019;33(3):93-103. [PMID: 30844304]
Korpela E., Dastgheyb R. M., Letendre S. L., et al. Longitudinal effects of polypharmacy on cognitive function in people with HIV. AIDS 2026;40(1):100-110. [PMID: 41065446]
Kovacs L., Kress T. C., Belin de Chantemele E. J. HIV, combination antiretroviral therapy, and vascular diseases in men and women. JACC Basic Transl Sci 2022;7(4):410-21. [PMID: 35540101]
Kulik G. L., Oliveira V. H. F., Wilson M. P., et al. Comparing the effectiveness of high intensity interval training vs continuous moderate intensity exercise on physical function among older adults with HIV. Open Forum Infect Dis 2026;13(1):ofag002. [PMID: 41583703]
Lazcano I., Ross R. D., Yin M. T. Updates on bone health in people living with HIV: global impact, prediction tools, and treatment. Curr Opin HIV AIDS 2025;20(4):331-36. [PMID: 40232833]
Livingston G., Huntley J., Liu K. Y., et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet 2024;404(10452):572-628. [PMID: 39096926]
Livio F., Deutschmann E., Moffa G., et al. Analysis of inappropriate prescribing in elderly patients of the Swiss HIV Cohort Study reveals gender inequity. J Antimicrob Chemother 2021;76(3):758-64. [PMID: 33279997]
Livio F., Marzolini C. Prescribing issues in older adults living with HIV: thinking beyond drug-drug interactions with antiretroviral drugs. Ther Adv Drug Saf 2019;10:2042098619880122. [PMID: 31620274]
Looby S. E. Clinical considerations for menopause and associated symptoms in women with HIV. Menopause 2023;30(3):329-31. [PMID: 36811963]
Machado S. Existential dimensions of surviving HIV: the experience of gay long-term survivors. J Hum Psychol 2012;52(1):6-29. https://doi.org/10.1177/0022167810389049
Maki P. M., Rubin L. H., Springer G., et al. Differences in cognitive function between women and men with HIV. J Acquir Immune Defic Syndr 2018;79(1):101-7. [PMID: 29847476]
Mallik I., Henderson M., Fidler S., et al. Aging of adult lifetime survivors with perinatal HIV. Curr Opin HIV AIDS 2025;20(4):379-87. [PMID: 40392284]
Masters M. C., Perez J., Wu K., et al. Baseline neurocognitive impairment (NCI) is associated with incident frailty but baseline frailty does not predict incident NCI in older persons with human immunodeficiency virus (HIV). Clin Infect Dis 2021;73(4):680-88. [PMID: 34398957]
Mendes de Leon K. F., Moody K., Nellen J. F., et al. Mode of administration matters: willingness of people with HIV to switch to future long-acting treatments, and health care professionals' intention to discuss these options. HIV Med 2025;26(9):1395-1404. [PMID: 40605247]
Molina J. M., Grund B., Gordin F., et al. Which HIV-infected adults with high CD4 T-cell counts benefit most from immediate initiation of antiretroviral therapy? A post-hoc subgroup analysis of the START trial. Lancet HIV 2018;5(4):e172-80. [PMID: 29352723]
Montoya J. L., Jankowski C. M., O'Brien K. K., et al. Evidence-informed practical recommendations for increasing physical activity among persons living with HIV. AIDS 2019;33(6):931-39. [PMID: 30946147]
Neupane N., Mehta M., Robinson-Papp J. Management of pain and other palliative needs in older people with HIV. Curr Opin HIV AIDS 2025;20(4):416-21. [PMID: 40232774]
Nightingale S., Ances B., Cinque P., et al. Cognitive impairment in people living with HIV: consensus recommendations for a new approach. Nat Rev Neurol 2023;19(7):424-33. [PMID: 37311873]
NYSDOH. New York State HIV/AIDS annual surveillance report for persons diagnosed through December 2024. 2025 Dec 1. https://www.health.ny.gov/diseases/aids/general/statistics/annual/2024/2024_annual_surveillance_report.pdf [accessed 2026 Mar 5]
O'Mahony D., Cherubini A., Guiteras A. R., et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3. Eur Geriatr Med 2023;14(4):625-32. [PMID: 37256475]
Palar K., Sheira L. A., Frongillo E. A., et al. Food is medicine for human immunodeficiency virus: improved health and hospitalizations in the Changing Health Through Food Support (CHEFS-HIV) Pragmatic Randomized Trial. J Infect Dis 2025;231(3):573-82. [PMID: 38696724]
Palella F. J., Hart R., Armon C., et al. Non-AIDS comorbidity burden differs by sex, race, and insurance type in aging adults in HIV care. AIDS 2019;33(15):2327-35. [PMID: 31764098]
Pellegrino R. A., Rebeiro P. F., Turner M., et al. Sex and race disparities in mortality and years of potential life lost among people with HIV: a 21-year observational cohort study. Open Forum Infect Dis 2023;10(1):ofac678. [PMID: 36726547]
Piggott D. A., Bandeen-Roche K., Mehta S. H., et al. Frailty transitions, inflammation, and mortality among persons aging with HIV infection and injection drug use. AIDS 2020;34(8):1217-25. [PMID: 32287069]
Pinholt E. M., Kroenke K., Hanley J. F., et al. Functional assessment of the elderly. A comparison of standard instruments with clinical judgment. Arch Intern Med 1987;147(3):484-88. [PMID: 3827424]
Quigley A., O'Brien K., Parker R., et al. Exercise and cognitive function in people living with HIV: a scoping review. Disabil Rehabil 2019;41(12):1384-95. [PMID: 29376434]
Rangaraj A., Connor S., Harding R., et al. Advanced HIV disease and health-related suffering--exploring the unmet need of palliative care. Lancet HIV 2023;10(2):e126-33. [PMID: 36427522]
Rubenstein L. Z., Alessi C. A., Josephson K. R., et al. A randomized trial of a screening, case finding, and referral system for older veterans in primary care. J Am Geriatr Soc 2007;55(2):166-74. [PMID: 17302651]
Saliba D., Elliott M., Rubenstein L. Z., et al. The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community. J Am Geriatr Soc 2001;49(12):1691-99. [PMID: 11844005]
Samji H., Cescon A., Hogg R. S., et al. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One 2013;8(12):e81355. [PMID: 24367482]
SeyedAlinaghi S., Mehraeen E., Mirzapour P., et al. Effectiveness of exercise on sarcopenia in HIV patients: a systematic review of current literature. AIDS Care 2025;37(3):349-61. [PMID: 39828981]
Singh H. K., Del Carmen T., Freeman R., et al. From one syndrome to many: incorporating geriatric consultation into HIV care. Clin Infect Dis 2017;65(3):501-6. [PMID: 28387803]
St Clair-Sullivan N., Bristowe K., Bremner S., et al. Comprehensive geriatric assessment for people living with HIV and frailty: a mixed-methods feasibility randomized controlled trial. HIV Med 2026;27(2):283-98. [PMID: 41271592]
Starup-Linde J., Rosendahl S. B., Storgaard M., et al. Management of osteoporosis in patients living with HIV-a systematic review and meta-analysis. J Acquir Immune Defic Syndr 2020;83(1):1-8. [PMID: 31809356]
Stone L., Looby S. E., Zanni M. V. Cardiovascular disease risk among women living with HIV in North America and Europe. Curr Opin HIV AIDS 2017;12(6):585-93. [PMID: 28832367]
Su T. T., O'Brien K. K., Zhabokritsky A., et al. The interplay of comorbidity, disability, and physical activity among older adults living with HIV: insights from the CHANGE HIV study. BMC Geriatr 2026;26(1):159. [PMID: 41495670]
Sukumaran L., Winston A., Marzolini C., et al. Polypharmacy in HIV: rethinking what counts and why it matters. HIV Med 2026;27(2):186-99. [PMID: 41121455]
Tamsukhin P. C., Bernardo R. M., Eti S. Palliative care considerations for the older adults with HIV/AIDS: a clinical practice review. Ann Palliat Med 2024;13(4):880-92. [PMID: 38735688]
Tariq S. Menopause: an opportunity to optimize health and well being for people with HIV. Curr Opin HIV AIDS 2025;20(4):388-95. [PMID: 40232823]
Tavoschi L., Gomes Dias J., Pharris A. New HIV diagnoses among adults aged 50 years or older in 31 European countries, 2004-15: an analysis of surveillance data. Lancet HIV 2017;4(11):e514-21. [PMID: 28967582]
Tinetti M., Huang A., Molnar F. The geriatrics 5M's: A new way of communicating what we do. J Am Geriatr Soc 2017;65(9):2115. [PMID: 28586122]
Tinetti M., Naik A. D., Dindo L., et al. Association of patient priorities-aligned decision-making with patient outcomes and ambulatory health care burden among older adults with multiple chronic conditions: a nonrandomized clinical trial. JAMA Intern Med 2019;179(12):1688-97. [PMID: 31589281]
Vance D. E., Rubin L. H., Valcour V., et al. Aging and neurocognitive functioning in HIV-infected women: a review of the literature involving the Women's Interagency HIV Study. Curr HIV/AIDS Rep 2016;13(6):399-411. [PMID: 27730446]
Varadarajan M., Blackburn S., Girometti N., et al. Implementation of a multidisciplinary approach to care for people with HIV aged 80 years and over. Int J STD AIDS 2025;36(1):65-71. [PMID: 39348909]
Verheij E., Boyd A., Wit F. W., et al. Long-term evolution of comorbidities and their disease burden in individuals with and without HIV as they age: analysis of the prospective AGE(h)IV cohort study. Lancet HIV 2023;10(3):e164-74. [PMID: 36774943]
Wallace C. G., Capriotti Z., Klase Z. HIV associated epigenetic trends and chronic diseases: insights into the hidden burden of chronic infection. Clin Epigenetics 2026;18(1):28. [PMID: 41546127]
Wandeler G., Johnson L. F., Egger M. Trends in life expectancy of HIV-positive adults on antiretroviral therapy across the globe: comparisons with general population. Curr Opin HIV AIDS 2016;11(5):492-500. [PMID: 27254748]
Winston A., Calcagno A., Cinque P. Cognitive impairment in persons with HIV: changing aetiologies and management strategies. Curr Opin HIV AIDS 2025;20(4):396-401. [PMID: 40298429]
Winston A., Spudich S. Cognitive disorders in people living with HIV. Lancet HIV 2020;7(7):e504-13. [PMID: 32621876]
Yarnall A. J., Sayer A. A., Clegg A., et al. New horizons in multimorbidity in older adults. Age Ageing 2017;46(6):882-88. [PMID: 28985248]
Yourman L. C., Lee S. J., Schonberg M. A., et al. Prognostic indices for older adults: a systematic review. JAMA 2012;307(2):182-92. [PMID: 22235089]
Zhabokritsky A., Falutz J. Frailty in people with HIV: a geriatric syndrome approach to aging with HIV. Curr Opin HIV AIDS 2025;20(4):344-49. [PMID: 40184515]
Zhang Y., He C., Peasgood T., et al. Use of quality-of-life instruments for people living with HIV: a global systematic review and meta-analysis. J Int AIDS Soc 2022;25(4):e25902. [PMID: 35396915]
Updates, Authorship, and Related Guidelines
| Updates, Authorship, and Related Guidelines | |
| Date of original publication | July 31, 2020 |
| Date of current publication | June 10, 2026 |
| Highlights of changes, additions, and updates in the June 10, 2026 edition |
Global: Updated discussion, references, and resources throughout guidance; incorporated long-term and lifetime survivors with HIV as target patient population |
| Intended users | Clinicians providing care to patients with HIV who are ≥50 years old or are long-term survivors |
| Lead author |
Eugenia L. Siegler, MD |
| Writing group |
Rona M. Vail, MD, AAHIVS; Sanjiv S. Shah, MD, MPH, AAHIVS; Steven M. Fine, MD, PhD; Joseph P. McGowan, MD, FACP, FIDSA, AAHIVS; Samuel T. Merrick, MD, FIDSA; Asa E. Radix, MD, MPH, PhD, FACP, AAHIVS; Anne K. Monroe, MD, MSPH; Jessica Rodrigues, MPH, MS; Christopher J. Hoffmann, MD, MPH, MSc, FACP; Brianna L. Norton, DO, MPH; Charles J. Gonzalez, MD |
| Author and writing group conflict of interest disclosures | There are no author or writing group conflict of interest disclosures. |
| Committee | |
| Developer and funder |
New York State Department of Health AIDS Institute (NYSDOH AI) |
| Development process |
See Guideline Development and Recommendation Ratings Scheme, below. |
| Related NYSDOH AI guidelines |
Guidelines
Guidance
Podcast |
Guideline Development and Recommendation Ratings
| Guideline Development: New York State Department of Health AIDS Institute Clinical Guidelines Program | |
| Program manager | Clinical Guidelines Program, Johns Hopkins University School of Medicine, Division of Infectious Diseases. See Program Leadership and Staff. |
| Mission | To produce and disseminate evidence-based, state-of-the-art clinical practice guidelines that establish uniform standards of care for practitioners who provide prevention or treatment of HIV, viral hepatitis, other sexually transmitted infections, and substance use disorders for adults throughout New York State in the wide array of settings in which those services are delivered. |
| Expert committees | The NYSDOH AI Medical Director invites and appoints committees of clinical and public health experts from throughout New York State to ensure that the guidelines are practical, immediately applicable, and meet the needs of care providers and stakeholders in all major regions of New York State, all relevant clinical practice settings, key New York State agencies, and community service organizations. |
| Committee structure |
|
| Disclosure and management of conflicts of interest |
|
| Evidence collection and review |
|
| Recommendation development |
|
| Review and approval process |
|
| External reviews |
|
| Update process |
|
| Recommendation Ratings Scheme | |||
| Strength | Quality of Evidence | ||
| Rating | Definition | Rating | Definition |
| A | Strong | 1 | Based on published results of at least 1 randomized clinical trial with clinical outcomes or validated laboratory endpoints. |
| B | Moderate | * | Based on either a self-evident conclusion; conclusive, published, in vitro data; or well-established practice that cannot be tested because ethics would preclude a clinical trial. |
| C | Optional | 2 | Based on published results of at least 1 well-designed, nonrandomized clinical trial or observational cohort study with long-term clinical outcomes. |
| 2† | Extrapolated from published results of well-designed studies (including nonrandomized clinical trials) conducted in populations other than those specifically addressed by a recommendation. The source(s) of the extrapolated evidence and the rationale for the extrapolation are provided in the guideline text. One example would be results of studies conducted predominantly in a subpopulation (e.g., one gender) that the committee determines to be generalizable to the population under consideration in the guideline. | ||
| 3 | Based on committee expert opinion, with rationale provided in the guideline text. | ||
Last updated on June 10, 2026